

Background. The Affordable Connectivity Program (ACP), established in 2021, provided eligible low-income households a monthly $30 internet subsidy. Despite its role in reducing digital disparities, only 40% of eligible households enrolled nationally. Link Health (LH), a Boston-based grassroots initiative, implemented a three-pillar (active, passive, and digital) outreach model to increase ACP uptake in Massachusetts and Texas.
Methods. From November 2022 to May 2024, LH partnered with community health centers in Boston and Houston to deliver on-site sign-up clinics (active approach), distribute multilingual printed materials (passive approach), and provide personalized text-message support (digital approach). Multilingual volunteers led screening and application filing, with follow-up via a dedicated helpline. Enrollment data were collected across 17 clinics and analyzed descriptively.
Results. Of approximately 9,774 individuals screened, 1,086 (11.1%) enrolled in the ACP. Enrollees were predominantly racial/ethnic minorities (78.9%), with 55.4% Hispanic/Latinx and 23.5% Black/African American. 68.4% of enrollees qualified for the ACP through current Medicaid enrollment, and 29.2% qualified through current SNAP enrollment. Digital sign-ups constituted 33.8% of enrollments. LH’s efforts distributed an estimated $390,960 in annual subsidies.
Conclusion. LH’s community-driven, three-pillar strategy bridged barriers to ACP enrollment. This model may inform future initiatives aimed at closing the digital divide and advancing health equity through targeted benefit enrollment.
Background
The Infrastructure Investment and Jobs Act, enacted in November 2021, allocated $14 billion to establish subsidies offering eligible households reduced rates for internet services within the framework of the Affordable Connectivity Program (ACP) [1]Federal Communications Commission. Affordable Connectivity Program. Federal Communications Commission. https://www.fcc.gov/affordable-connectivity-program. Accessed April 15, 2025..
As a result of the COVID-19 pandemic, regulations were altered to facilitate improvement in telehealth as an important health care modality [2]Telehealth policy changes after the COVID-19 public health emergency | Telehealth.HHS.gov. Accessed October 21, 2024. https://telehealth.hhs.gov/providers/telehealth-policy/policy-changes-after-the-covid-19-public-health-emergency. Telehealth offered high promises of enabling healthcare providers to consult with patients remotely, manage chronic conditions, and deliver public health education—actions that help preserve hospital resources for the most urgent cases [3]Demeke HB. Trends in Use of Telehealth Among Health Centers During the COVID-19 Pandemic — United States, June 26–November 6, 2020. MMWR Morbidity and Mortality Weekly Report. 2021;70(7). doi:https://doi.org/10.15585/mmwr.mm7007a3. However, a nationwide digital divide hampered potential benefits of telehealth expansion; disparities in internet access meant patients were left behind, unable to access telehealth [4]Eruchalu CN, Pichardo MS, Bharadwaj M, et al. The Expanding Digital Divide: Digital Health Access Inequities during the COVID-19 Pandemic in New York City. J Urban Health. 2021;98(2):183-186. doi:10.1007/s11524-020-00508-9,[5]Dolcini MM, Canchola JA, Catania JA, et al. National-Level Disparities in Internet Access Among Low-Income and Black and Hispanic Youth: Current Population Survey. J Med Internet Res. 2021;23(10):e27723. doi:10.2196/27723,[6]Saeed SA, Masters RM. Disparities in Health Care and the Digital Divide. Curr Psychiatry Rep. 2021;23(9):61. doi:10.1007/s11920-021-01274-4. The American Medical Association (AMA) identified broadband access as impacting several social determinants of health domains, subsequently influencing health outcomes and worsening health disparities [7]Benda NC, Veinot TC, Sieck CJ, Ancker JS. Broadband Internet Access Is a Social Determinant of Health! American Journal of Public Health. 2020;110(8):1123-1125. doi:https://doi.org/10.2105/ajph.2020.305784. Patients without internet access are often the most vulnerable; those disconnected experience disproportionately worse health outcomes [8]Marzouk S, Velasquez DE, Joseph N, Martin A. Broadband for better health-ensuring internet access for all. BMJ. 2023 Jul 20;382:1673. doi: 10.1136/bmj.p1673. PMID: 37474205.—this trend underscores the vital importance of the ACP and similar programs, demonstrating how enhancing digital connectivity may serve as an efficient leverage point to improve health outcomes by simultaneously targeting multiple social determinants of health. .
Through the ACP, individuals receiving assistance from the Supplemental Nutrition Assistance Program (SNAP), or those whose income was less than twice the federal poverty threshold, were qualified to obtain a monthly subsidy of $30 to cover costs associated with packages from internet service providers (ISPs), and a $100 subsidy for acquisition of a tablet or laptop [9]Affordable Connectivity Program | Federal Communications Commission. Accessed October 21, 2024. https://www.fcc.gov/acp. Funds for the ACP expired in June 2024, but its impact was profound, enabling over 23 million households to connect to internet and telehealth services [10]Layton R. Policy No-Brainer: Extend The Affordable Connectivity Program For 5 Years With $30 Billion. Forbes. Accessed October 21, 2024. https://www.forbes.com/sites/roslynlayton/2022/09/30/policy-no-brainer-extend-the-affordable-connectivity-program-for-5-years-with-30-billion/,[11]House TW. FACT SHEET: As Affordable Connectivity Program Hits Milestone of Providing Affordable High-Speed Internet To 23 Million Households Nationwide, Biden-Harris Administration Calls on Congress to Extend Its Funding. The White House. February 6, 2024. Accessed November 11, 2024. https://www.whitehouse.gov/briefing-room/statements-releases/2024/02/06/fact-sheet-as-affordable-connectivity-program-hits-milestone-of-providing-affordable-high-speed-internet-to-23-million-households-nationwide-biden-harris-administration-calls-on-congress-t/.
Despite the ACP’s role in closing gaps in access to wireless internet, its uptake varied, with some states and counties observing higher levels than others. Data from the Universal Service Administrative Company showed 19.6 million of 48.6 million eligible households enrolled nationwide [12]Affordable Connectivity Program. Universal Service Administrative Company. Accessed October 21, 2024. https://www.usac.org/about/affordable-connectivity-program/,[13]Persons in Low-Income Households Have Less Access to Internet Services. ASPE. March 22, 2021. Accessed October 21, 2024. https://aspe.hhs.gov/reports/low-income-internet-access. Community-based organizations played a critical role in the effort to reduce enrollment barriers, which include a lack of awareness or trust, and challenges in completing application forms. Without state funding, local partnership, or philanthropy to power enrollment initiatives, those in need of benefits would be left without the opportunity to sign-up [14]State and Local Leaders Can Close Digital Divide by Removing Barriers to Free Internet, Says EducationSuperHighway. EducationSuperHighway. Accessed April 28, 2025. https://www.educationsuperhighway.org/announcements/state-and-local-leaders-can-close-digital-divide-by-removing-barriers-to-free-internet-says-educationsuperhighway/. Link Health (LH), a Boston-based grassroots initiative established in 2021, aimed to increase uptake of the ACP and address established drivers of digital health disparities, including difficulty navigating the health care system, communication difficulties from language barriers, and mistrust of providers [5]Dolcini MM, Canchola JA, Catania JA, et al. National-Level Disparities in Internet Access Among Low-Income and Black and Hispanic Youth: Current Population Survey. J Med Internet Res. 2021;23(10):e27723. doi:10.2196/27723 through a community-driven approach. We hypothesize that LH functions as a model for connecting patients to internet services, and that it does so by reducing communication gaps and administrative challenges that arise between qualifying populations and ISPs.
Methods
Recruitment & Preparation
LH employed a three-pillar approach of active, passive, and digital methods through on-site, health center-based sign-up clinics, dissemination of instructional materials, and personalized digital support. The approach prioritized addressing three obstacles: 1) awareness of the ACP, 2) technical issues with registration and eligibility, and 3) language barriers.
To empower communities and lessen mistrust among individuals within them, LH team members were recruited from the areas it served. The program commenced operations in partnership with East Boston Neighborhood Health Center and South End Community Health Center (now collectively called NeighborHealth), Massachusetts General Hospital (MGH), and the Dimock Center in Boston, as well as the Legacy Community Health Center network in Houston. By creating local partnerships with community-based organizations and a team of diverse stakeholders and leaders, LH was integrated into the community.
Weekly clinics were coordinated by a field director. A data manager oversaw data intake and integration across the three-pillar approach. A volunteer coordinator used email communication to recruit members from neighboring healthcare facilities and medical schools to serve on-site as ACP sign-up volunteers; this is represented in Figure 1 as the “White Coat” on-site. White Coats were recruited based on relationships between LH and specific institutions within Boston and Houston. The presence of medical providers and trainees provided credibility, as they could share knowledge on the relationship between broadband connectivity and other health determinants. The White Coats worked voluntarily. Successful communication was key in facilitating ACP sign-up, given the application’s length, and so multilingual volunteers were recruited to ensure accessibility for non-English speakers.
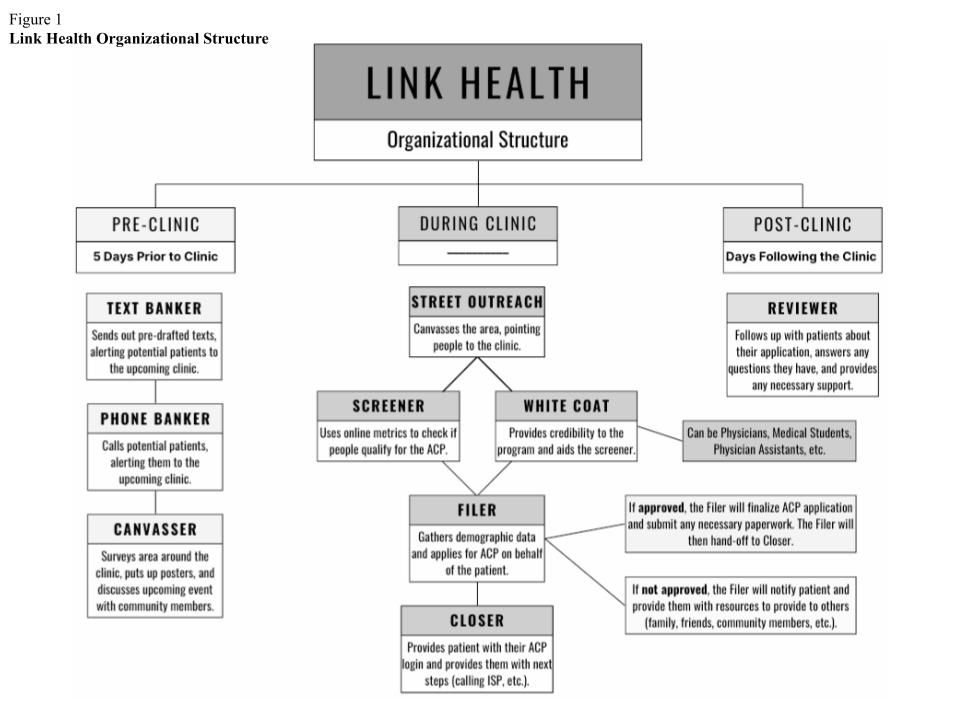
Figure 1 Link Health Organizational Structure
The Three-Pillar Approach
Active Approach
LH’s partnerships helped streamline ACP enrollment. Through collaboration between community organizers and volunteers, a political campaign model was used to carry out place-based, in-person sign-ups for the ACP. Community organizers used knowledge of the target community and get-out-the-vote strategies to connect with difficult-to-reach populations and increase enrollment. These strategies involve shareable social media messages, printable “prescriptions” with instructions, and in-person registration tables [15]Junior JA, Ha YP, Ruxin TR, et al. A National Voter Registration Campaign. Pediatrics. 2023;152(2):e2022059501. doi:10.1542/peds.2022-059501.
Twice a week, in-person registration events were held at health centers located within Boston and Houston neighborhoods. Visitors to and patients of the clinics often belonged to low-income, immigrant households. The primary languages spoken included Spanish, English, Creole dialects, and Portuguese. These centers were interested in LH’s endeavor and in the ACP, as these partnerships offered additional patient navigation services and the potential of increasing telehealth utilization. This active approach operated on a three-step sequence: pre-clinic, clinic, and post-clinic (Figure 1).
Pre-clinic phase. Approximately five days before the in-person clinic, LH launched the “pre-clinic phase.” This phase was comprised of 1) raising awareness of the event through text and phone banking, social media, and canvassing, 2) organizing the appropriate number of LH staff and volunteers to handle the demand of the clinic location (3-10 per clinic), and 3) preparing discharge handouts to facilitate sign-ups and engagement.
Clinic phase. On the day of the event, the “clinic phase” took place. The White Coats arrived at the clinic along with LH staff to assist patients signing up for the ACP. Volunteers were assigned the following roles: Street Outreach, Screener, Filer, and Closer (Figure 1). This team communicated the importance of internet accessibility to patients and community members during downtime in waiting rooms and outside the clinic. These conversations, intended to build rapport, took place in clinics staffed by individuals who reflected the community's cultural makeup.
After welcoming conversations, volunteers facilitated a handoff to LH staff trained to complete ACP sign-ups, or, if the patient lacked time to sign-up, provided them with a printed resource, such as fictitious $30 handouts (reflecting the value of the ACP benefit). The Screener asked the patient a series of questions to verify eligibility for the ACP and then worked with a White Coat to highlight how the ACP supports healthcare participation. If the patient was eligible, they were directed to the Filer, who gathered necessary information to complete the ACP application on the patient’s behalf. If approved, the Closer provided log-in information to the ACP account and explained next steps involving the ISPs. If more information was required to prove eligibility, the patient was connected with the digital approach team.
Post-clinic phase. The “post-clinic phase” provided patients additional support with their application. Digital LH staff contacted patients who had technical issues or who were not approved. All individuals registered for the ACP were provided a dedicated helpline number, which was overseen by LH personnel and used to address outstanding questions.
Passive approach
LH’s passive approach involved disseminating handouts and discharge paperwork to promote sign-ups. By distributing these items, LH provided tools to sign up for the ACP independently. To raise awareness of the ACP in a high-volume setting such as the MGH Emergency Department, information was spread by sharing the same documents.
To ensure these materials were widely accessible, the common languages spoken in LH service locations were identified, and the team subsequently worked with the We Got Us Project to translate the documents into six languages (Haitian Creole, Chinese, Tagalog, Somali, Portuguese, and Vietnamese).
Digital approach
The final piece to the three-pillar approach was to contact patients through text-messaging. Text-messaging equipped LH to assist with virtual ACP sign-ups and to provide patients long-term support. Multilingual digital navigators processed sign-ups and sent personalized text-messages to patients. This approach increased the likelihood that each patient who started their application would receive their benefit. Virtual support also allowed patients to engage in this process at their convenience.
The digital approach was curated in response to technical issues on the ACP website that prevented individuals from qualifying for benefits. Instances were seen in which individuals who had already qualified for other benefit programs became frustrated by the website’s need for additional verification. This resulted in prolonged waiting between application submission and benefit receipt. The digital approach allowed patients to remain connected with LH.
Approvals & Data Collection
The research protocol for this work was reviewed by the Institutional Review Board (IRB) of the Northeastern University School of Nursing (IRB #: 24-10-06) and determined to be exempt from further IRB oversight.
Data were collected in-person across 13 clinics in Boston and four clinics in Houston and digitally from November 2022 to May 2024. To estimate the funding LH distributed annually, the total number of enrollments was multiplied by the monthly benefit ($30) and number of months in a year (12). Descriptive statistics and figures were generated via R 4.3.1.
Results
Enrollment occurred from November 2022 through May 2024 across 17 clinics in Massachusetts and Texas. Over 9,774 patients were screened for ACP eligibility. LH’s efforts yielded the enrollment of 1,086 patients into the ACP, as illustrated in Table 1 and Figure 2.
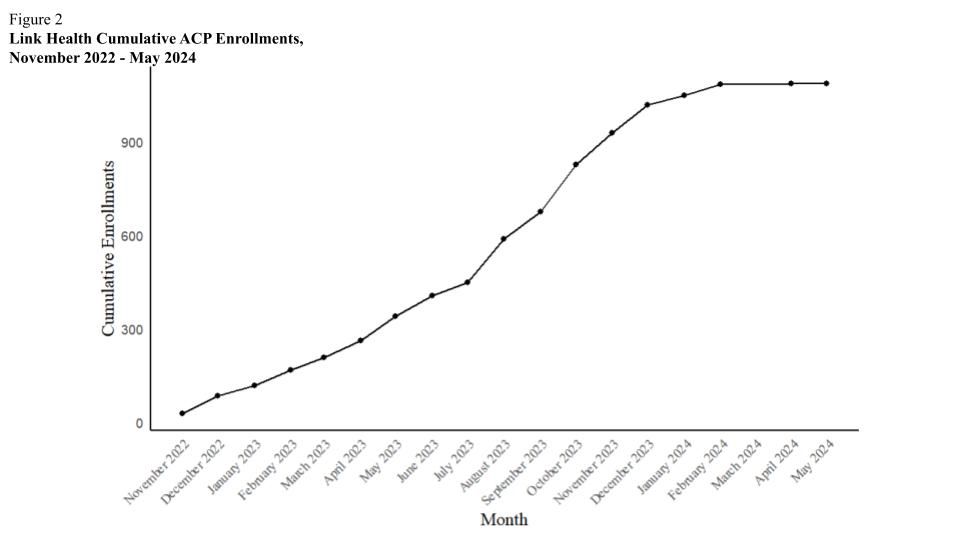
Figure 2 Link Health Cumulative ACP Enrollments, November 2022 - May 2024
No. (%) |
Overall (n = 1086) |
Massachusetts (n = 715) |
Texas (n = 363) |
Other (n = 8) |
|---|---|---|---|---|
Race/Ethnicity |
||||
Hispanic/Latinx |
602 (55.4) |
412 (57.6) |
188 (51.8) |
2 (25.0) |
Black/African American |
255 (23.5) |
153 (21.4) |
101 (27.8) |
1 (12.5) |
White |
142 (13.1) |
96 (13.4) |
43 (11.8) |
3 (37.5) |
Asian |
32 (2.9) |
22 (3.1) |
10 (2.8) |
0 (0.0) |
Prefer Not to Say |
27 (2.5) |
11 (1.5) |
15 (4.1) |
1 (12.5) |
Other |
28 (2.6) |
21 (2.9) |
6 (1.6) |
1 (12.5) |
Sex |
||||
Male |
401 (36.9) |
276 (38.6) |
120 (33.0) |
5 (62.5) |
Female |
681 (62.7) |
437 (61.1) |
241 (66.4) |
3 (37.5) |
Other |
4 (0.4) |
2 (0.3) |
2 (0.6) |
0 (0.0) |
Age Ranges |
||||
Under 18 |
24 (2.2) |
12 (1.7) |
11 (3.0) |
1 (12.5) |
18-36 |
312 (28.7) |
174 (24.3) |
137 (37.7) |
1 (12.5) |
37-55 |
425 (39.1) |
285 (39.9) |
136 (37.5) |
4 (50.0) |
55 and over |
325 (29.9) |
244 (34.1) |
79 (21.8) |
2 (25.0) |
Qualifying Meansa |
||||
Medicaid |
743 (68.4) |
472 (66.0) |
266 (73.3) |
5 (62.5) |
Medicare |
144 (13.3) |
113 (15.8) |
30 (8.3) |
1 (12.5) |
SNAP |
317 (29.2) |
280 (29.2) |
33 (9.1) |
4 (50.0) |
WIC |
81 (7.5) |
47 (6.6) |
34 (9.4) |
0 (0.0) |
Income |
109 (10.0) |
66 (9.2) |
40 (11.0) |
3 (37.5) |
SSI |
83 (7.6) |
69 (9.7) |
12 (3.3) |
2 (25.0) |
Federal Public Housing Assistance |
61 (5.6) |
55 (7.7) |
5 (1.4) |
1 (12.5) |
Pell Grant |
7 (0.6) |
6 (0.8) |
1 (0.3) |
0 (0.0) |
Free or Reduced Lunch |
53 (4.9) |
27 (3.8) |
25 (6.9) |
1 (12.5) |
Veteran’s/Survivor’s Pension |
5 (0.5) |
3 (0.4) |
2 (0.6) |
0 (0.0) |
aSome individuals qualified for the ACP by multiple means, therefore percentages may add to over 100.
Abbreviations: ACP, Affordable Connectivity Program; SNAP, Supplemental Nutrition Assistance Program; WIC, Women, Infants, & Children Nutrition Program; SSI, Supplemental Security Income.
Among 1,086 enrollees, 367 patients enrolled via the digital platform, while the remaining patients enrolled through the active or passive approach. A significant proportion of ACP beneficiaries were found to be eligible via Medicaid (n = 743, 68.4%), followed by SNAP (n = 317, 29.2%). Those belonging to a racial or ethnic minority group numbered 857 (78.9%), with 602 (55.4%) identifying as Hispanic/Latinx and 255 (23.5%) as Black/African American. Across outreach methods, LH disbursed an estimated $390,960 annually to patients of partner community sites and attendees of in-person sign-up clinics, which included health center patients and bystanders.
Conclusion
This report highlights LH’s active, passive, and digital enrollment strategy to facilitate ACP sign-up. LH’s three-pillar model offers a framework for organizations aiming to bridge the digital divide and connect underserved communities to benefit programs like the ACP. There remains an urgent need for continued investment in safety-net programs like the ACP. As of 2022, 18.8% of households in Suffolk County, Massachusetts lacked a desktop or laptop, and 30.1% did not use the internet at broadband speeds. In Harris County, Texas, the figures were 22.0% and 32.3%, respectively [16]Power BI Report. Accessed November 11, 2024. https://msit.powerbi.com/view?r=eyJrIjoiMmUyMzY2YjUtNDdmMS00ZTYyLThhMDAtMTUxMmZmNTcxMGE0IiwidCI6IjcyZjk4OGJmLTg2ZjEtNDFhZi05MWFiLTJkN2NkMDExZGI0NyIsImMiOjV9. These gaps highlight persistent inequities in accessing digital services, even in urban areas. This gap widens when comparing affluent locales to poorer ones [17]Exacerbating the divide? Investigating rural inequalities in high speed broadband availability. Accessed July 11, 2025. https://www.esri.ie/publications/exacerbating-the-divide-investigating-rural-inequalities-in-high-speed-broadband, which concentrate in urban regions such as those in Suffolk County and Harris County. As digital access is key to job-seeking, work-from-home opportunities, telehealth, and myriad day-to-day activities, communities must cultivate the capacity for their members to connect to these services.
There are limitations to LH’s approach and evaluation. First, important post-ACP registration outcomes, including benefit receipt and device acquisition, were not tracked. A partnership with the National Verifier, which administers the ACP, might have enabled a secondary analysis of these data. While we recognize this shortcoming, LH appreciated the urgency with which individuals need broadband services, and formal relationships with administering agencies take significant periods of time to foster. Additionally, these partnerships depend on providing proof-of-concept, such that LH first needed to establish its capacity for signing patients up for benefits. Organizations looking to adopt LH’s three-pillar approach would benefit from identifying effective means to survey patients post-enrollment regarding benefit receipt, while recognizing challenges inherent in obtaining accurate data from self-reported benefit receipt.
Second, LH did not record the number of ineligible patients or distinguish between passive and active enrollments, limiting comparative analysis.
Third, some potentially eligible patients were not screened. While encounters with the team were brief, many patients were visiting the clinic for other appointments and were unable to devote time to complete ACP registration. Comfort in providing personal identifying information to the LH team is another barrier; while the team sought to quell anxieties with multilingual staff who established credibility as working with the clinics, providing personal information may have been unnerving. Lastly, if registration was not completed in the clinic, a patient’s preexisting barriers to communication technology may have impeded follow-up with the digital team.
Fourth, although LH emphasized access to telehealth as a benefit of ACP enrollment, access to internet services does not imply increased engagement with telehealth. LH can integrate clinics’ medical records to monitor patient telehealth utilization following enrollment in broadband connectivity programs; this could be compared against a control group that did not sign-up.
Another study could investigate enrollment in the ACP based on income or educational status; this could help provide insight into whether enrollees experience barriers to sign-up based on other health determinants.
While downstream utilization metrics such as telehealth engagement are difficult to measure, LH’s influence on ACP enrollments is unequivocal: over 1,000 individuals were enrolled. This effort addressed barriers to access, including knowledge of the program and administrative burden.
LH’s three-pillar approach demonstrated that community-based events that foster trust might help close the gap between vulnerable communities and digital access. In the future, a greater breadth of basic needs can be addressed through adding additional benefit programs to LH’s repertoire. Increasing partnerships with community representatives and program administrators can bolster organizational credibility, reach to neighborhoods, and improve the ability to monitor how enrollment in these programs affects health outcomes.
Acknowledgments
All authors made substantive contributions to the conception and design of the work. All authors were involved in drafting and reviewing the work critically for intellectual content. All authors provided final approval of the version to be submitted and agreed to be accountable for all aspects of the work, including ensuring questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
Funding/Support
City of Boston and State of Massachusetts.
Other disclosures
None.
Declarations
Ethics approval and consent to participate
The manuscript reports that the Northeastern University School of Nursing Institutional Review Board reviewed the protocol (IRB #: 24-10-06) and determined it to be exempt from further IRB oversight.
Consent for publication
Not reported in the submitted manuscript. Confirm whether consent was waived or not applicable under the IRB exemption before final PMC packaging.
Availability of data and materials
The operational enrollment data analyzed in this article are not publicly available. De-identified summary data may be available from the corresponding author on reasonable request, subject to applicable privacy and institutional constraints.
Competing interests
The authors declare no commercial or financial conflict of interest.
Authors' contributions
Nicholos P Joseph: Writing - original draft; Writing - review and editing; Conceptualization | Timothy Scheinert: Writing - original draft; Writing - review and editing; Supervision | Ashley K Roth: Writing - original draft; Writing - review and editing | Reese Joy Fields Green: Writing - original draft; Writing - review and editing; Visualization; Data curation | Dominick Contreras: Writing - original draft; Writing - review and editing | Ahmad Hider: Writing - original draft; Writing - review and editing | Alister Martin: Writing - original draft; Writing - review and editing; Supervision; Project administration; Conceptualization
References
- Federal Communications Commission. Affordable Connectivity Program. Federal Communications Commission. https://www.fcc.gov/affordable-connectivity-program. Accessed April 15, 2025.
- Telehealth policy changes after the COVID-19 public health emergency | Telehealth.HHS.gov. Accessed October 21, 2024. https://telehealth.hhs.gov/providers/telehealth-policy/policy-changes-after-the-covid-19-public-health-emergency
- Demeke HB. Trends in Use of Telehealth Among Health Centers During the COVID-19 Pandemic — United States, June 26–November 6, 2020. MMWR Morbidity and Mortality Weekly Report. 2021;70(7). doi:https://doi.org/10.15585/mmwr.mm7007a3
- Eruchalu CN, Pichardo MS, Bharadwaj M, et al. The Expanding Digital Divide: Digital Health Access Inequities during the COVID-19 Pandemic in New York City. J Urban Health. 2021;98(2):183-186. doi:10.1007/s11524-020-00508-9
- Dolcini MM, Canchola JA, Catania JA, et al. National-Level Disparities in Internet Access Among Low-Income and Black and Hispanic Youth: Current Population Survey. J Med Internet Res. 2021;23(10):e27723. doi:10.2196/27723
- Saeed SA, Masters RM. Disparities in Health Care and the Digital Divide. Curr Psychiatry Rep. 2021;23(9):61. doi:10.1007/s11920-021-01274-4
- Benda NC, Veinot TC, Sieck CJ, Ancker JS. Broadband Internet Access Is a Social Determinant of Health! American Journal of Public Health. 2020;110(8):1123-1125. doi:https://doi.org/10.2105/ajph.2020.305784
- Marzouk S, Velasquez DE, Joseph N, Martin A. Broadband for better health-ensuring internet access for all. BMJ. 2023 Jul 20;382:1673. doi: 10.1136/bmj.p1673. PMID: 37474205.
- Affordable Connectivity Program | Federal Communications Commission. Accessed October 21, 2024. https://www.fcc.gov/acp
- Layton R. Policy No-Brainer: Extend The Affordable Connectivity Program For 5 Years With $30 Billion. Forbes. Accessed October 21, 2024. https://www.forbes.com/sites/roslynlayton/2022/09/30/policy-no-brainer-extend-the-affordable-connectivity-program-for-5-years-with-30-billion/
- House TW. FACT SHEET: As Affordable Connectivity Program Hits Milestone of Providing Affordable High-Speed Internet To 23 Million Households Nationwide, Biden-Harris Administration Calls on Congress to Extend Its Funding. The White House. February 6, 2024. Accessed November 11, 2024. https://www.whitehouse.gov/briefing-room/statements-releases/2024/02/06/fact-sheet-as-affordable-connectivity-program-hits-milestone-of-providing-affordable-high-speed-internet-to-23-million-households-nationwide-biden-harris-administration-calls-on-congress-t/
- Affordable Connectivity Program. Universal Service Administrative Company. Accessed October 21, 2024. https://www.usac.org/about/affordable-connectivity-program/
- Persons in Low-Income Households Have Less Access to Internet Services. ASPE. March 22, 2021. Accessed October 21, 2024. https://aspe.hhs.gov/reports/low-income-internet-access
- State and Local Leaders Can Close Digital Divide by Removing Barriers to Free Internet, Says EducationSuperHighway. EducationSuperHighway. Accessed April 28, 2025. https://www.educationsuperhighway.org/announcements/state-and-local-leaders-can-close-digital-divide-by-removing-barriers-to-free-internet-says-educationsuperhighway/
- Junior JA, Ha YP, Ruxin TR, et al. A National Voter Registration Campaign. Pediatrics. 2023;152(2):e2022059501. doi:10.1542/peds.2022-059501
- Power BI Report. Accessed November 11, 2024. https://msit.powerbi.com/view?r=eyJrIjoiMmUyMzY2YjUtNDdmMS00ZTYyLThhMDAtMTUxMmZmNTcxMGE0IiwidCI6IjcyZjk4OGJmLTg2ZjEtNDFhZi05MWFiLTJkN2NkMDExZGI0NyIsImMiOjV9
- Exacerbating the divide? Investigating rural inequalities in high speed broadband availability. Accessed July 11, 2025. https://www.esri.ie/publications/exacerbating-the-divide-investigating-rural-inequalities-in-high-speed-broadband.