


ABSTRACT
Background
Hospital environments significantly impact pediatric patients’ physical and emotional well-being. However, conventional hospital designs often fail to integrate child-friendly engagement strategies, leading to increased anxiety, reduced caregiver satisfaction, and operational inefficiencies. The HackPeds clinical audit, grounded in a continuous quality improvement framework, evaluated pediatric healthcare spaces at Evercare Hospital Lahore to identify systemic gaps and implement targeted interventions over a structured audit cycle.
Methods
A two-phase clinical audit was conducted at Evercare Hospital Lahore, with an initial assessment in November 2024, followed by a structured re-audit in January 2025, allowing for approximately three months of intervention implementation. The assessment was inspired by Joint Commission International and similar global pediatric care standards while also incorporating human-centered design principles. A checklist-based facility evaluation, structured staff interviews, and real-time benchmarking against best practices were used. The auditor, a pediatrician, emergency medicine consultant, and health innovation expert, assessed spatial utilization, caregiver engagement, and pediatric emergency preparedness, among other factors.
Results
The initial audit identified underutilized pediatric spaces, lack of interactive play zones, inconsistent emergency preparedness, and inadequate staff training in play therapy. Over the three-month intervention period, structured play areas were introduced, pediatric emergency response protocols were strengthened, and caregiver education initiatives were expanded. The January 2025 re-audit showed improvements in the use of engagement spaces, staff preparedness, and caregiver participation in pediatric care activities, although gaps remained in optimizing space utilization and embedding structured storytelling interventions.
Conclusion
By embedding continuous quality improvement strategies and structured re-audit cycles, HackPeds provides a scalable framework for pediatric healthcare transformation. The model is positioned for multi-site validation across Evercare Group hospitals in Nigeria and Kenya, with potential for broader adaptation in global pediatric healthcare settings. Future audits will assess longitudinal impact and sustainability to optimize pediatric patient experience, caregiver engagement, and emergency preparedness.
Keywords: Pediatric hospital design, clinical audit, quality improvement, human-centered design, play therapy, storytelling in healthcare, pediatric emergency care, caregiver engagement, healthcare innovation, global health scalability.
BACKGROUND
Hospital environments are integral to pediatric healthcare, influencing not only clinical outcomes but also psychosocial well-being. Conventional hospital designs often prioritize medical efficiency over pediatric and family-centered design thinking, leading to increased anxiety, reduced caregiver engagement, and suboptimal patient experiences [1]Bock EP, Nilsson S, Jansson PA, et al. Literature review: evidence-based health outcomes and perceptions of the built environment in pediatric hospital facilities. J Pediatr Nurs. 2021;61:e42-e50. doi:10.1016/j.pedn.2021.04.013-[3]Phuria S. The role of hospital design in improving patient recovery. Int J Adv Res. 2024;12:670-675. doi:10.21474/IJAR01/19499. Research highlights that child-friendly spaces incorporating sensory engagement, storytelling interventions, and structured play zones can reduce procedural distress, enhance health literacy, and improve overall satisfaction [4]Bole A, Bernstein A, White MJ; Council on Environmental Health and Climate Change; Section on Minority Health, Equity, and Inclusion. The built environment and pediatric health. Pediatrics. 2024;153(1):e2023064772. doi:10.1542/peds.2023-064772-[7]Laursen J, Danielsen A, Rosenberg J. Effects of environmental design on patient outcome: a systematic review. HERD. 2014;7(4):108-119. doi:10.1177/193758671400700410 .
Despite these insights, empirical validation of pediatric hospital design innovations remains limited, particularly in low- and middle-income countries (LMICs) where resource constraints influence care delivery [1]Bock EP, Nilsson S, Jansson PA, et al. Literature review: evidence-based health outcomes and perceptions of the built environment in pediatric hospital facilities. J Pediatr Nurs. 2021;61:e42-e50. doi:10.1016/j.pedn.2021.04.013, [6]Gaminiesfahani H, Lozanovska M, Tucker R. A scoping review of the impact on children of the built environment design characteristics of healing spaces. HERD. 2020;13(4):98-114. doi:10.1177/1937586720903845. Prior work from Pakistan and other LMIC settings has demonstrated the importance of integrating child-friendly engagement strategies into hospital workflows. Initiatives such as storytelling-based health literacy programs [8]Butt W, Mustafa F, Ahsan Z, Salim S, Tahir H, Mian A. The immunization questionnaire for understanding unwellness (TIQUU): fun learning about vaccination using an innovative storytelling approach. Vacunas (Engl Ed). 2024;25:304-312. doi:10.1016/j.vacune.2024.08.002, [9]Ahmad H, Naeem R, Feroze A, et al. Teaching children road safety through storybooks: an approach to child health literacy in Pakistan. BMC Pediatr. 2018;18(1):31. doi:10.1186/s12887-018-0982-5 and hospital-based pediatric innovation models [10]Farooqi W, Subhani F, Mian A. Paediatric innovation in Pakistan: our experience and a call to action. Arch Dis Child. 2017;102(10):963-967. doi:10.1136/archdischild-2016-312123, [11]Madhani S, Farooqi WH, Mian AI. Stimulating innovation through the hackathon concept in paediatrics: our experience at the Aga Khan University. Arch Dis Child. 2017;102(10):994. doi:10.1136/archdischild-2017-313648 have shown potential for improving child engagement, caregiver participation, and provider-patient communication. Additionally, research on pediatric emergency care streamlining in LMIC settings underscores the need for structured audit mechanisms to assess and refine pediatric healthcare spaces [12]Bhimani S, Brown N, Mian AI. Streamlining pediatric emergency medicine at a tertiary-care hospital of a low- to middle-income country. Indian Pediatr. 2015;52:1021-1024. Accessed March 24, 2025. https://indianpediatrics.net/dec2015/dec-1021-1024.htm.
Building on this foundation, this study applies a structured clinical audit framework to pediatric hospital design, embedding continuous quality improvement principles into pediatric care environments. Unlike static infrastructural recommendations, this approach integrates pediatric and family-centered design thinking, caregiver engagement strategies, and distraction-based storytelling interventions to create measurable, scalable improvements in pediatric patient experience.
To operationalize these principles, the HackPeds innovation framework was developed by Innovly, an innovation management startup, to apply structured clinical audits for pediatric and other hospital units’ design assessment [13]Innovly. (2025, March 11). Innovly: Healthcare innovation platform. https://innovly.net/. This study implemented a pediatric audit innovation at Evercare Hospital Lahore, with the goal to identify systemic gaps, implement targeted interventions, and measure early-stage improvements in pediatric engagement, spatial utilization, and emergency preparedness.
This study does not merely explore pediatric hospital design in isolation but positions it as a dynamic, interactive component of care delivery. By aligning with ongoing work in child health literacy, patient distraction methodologies, and structured pediatric engagement, it provides a scalable, data-driven framework for optimizing pediatric hospital environments in diverse healthcare settings. The findings will inform multi-site validation in Evercare hospitals in Nigeria and Kenya, with the potential for broader global application in pediatric healthcare transformation.
METHODS
Study Design and Setting
This study employed a structured, two-phase clinical audit to evaluate pediatric inpatient (IPD) and outpatient (OPD) environments at Evercare Hospital Lahore (EHL). The baseline audit was conducted in November 2024, followed by a structured re-audit in January 2025 to assess the impact of targeted interventions over an approximately three-month period. This continuous quality improvement (CQI)-driven approach ensured that the evaluation was not a one-time assessment but an iterative, data-informed process aimed at refining pediatric care environments.
EHL is a 270-bedded tertiary-care hospital that is part of the Evercare Group, a global healthcare network operating in South Asia and Africa, with hospitals in Pakistan, Kenya, and Nigeria. Evercare focuses on high-quality, accessible healthcare in emerging markets and is accredited by leading quality and safety frameworks [14]Evercare Group. (2025, March 11). Evercare Group: Transforming healthcare. https://www.evercaregroup.com/. EHL specifically provides comprehensive pediatric care, including emergency services, neonatal and pediatric intensive care, and outpatient specialty clinics [15]Evercare Hospital Lahore. (2025, March 11). Evercare Hospital Lahore. https://www.evercarehospitallahore.com/.
The HackPeds innovation framework, developed by Innovly, an innovation management startup, provided the structured methodology for this audit. Innovly has developed unit-specific clinical audit innovations for emergency departments, ICUs, and other high-risk hospital spaces [13]Innovly. (2025, March 11). Innovly: Healthcare innovation platform. https://innovly.net/. These include EmTEx (focused on emergency medicine) and CritiCore (for critical care/ICU environments), which are currently under review for publication. The HackPeds framework builds upon this expertise by integrating pediatric and family-centered design thinking into structured clinical assessments of hospital environments. HackPeds has also been implemented in Nigeria, with findings from that audit currently being prepared for publication.
Audit Conductor and Data Collection
The audit was conducted by a single senior clinician, also the senior author of this paper (Dr. Asad Mian), with expertise in pediatrics, emergency medicine, and healthcare innovation. This individual was responsible for assessing clinical safety, pediatric engagement strategies, hospital design, and emergency preparedness, ensuring a comprehensive and multidisciplinary evaluation within a single framework. The EHL patient safety, quality, and experience team provided logistical and technical support when necessary, particularly for accessing institutional performance metrics and facilitating structured walkthroughs. However, to minimize bias, EHL team members did not serve as interviewers and were not involved in direct data collection or qualitative analysis.
Data collection involved a combination of checklist-based facility assessments, structured staff interviews, and facility walkthroughs to ensure a holistic review of pediatric care environments. Findings from the baseline audit in November 2024 were compared with those from the January 2025 re-audit, capturing both initial gaps and measurable improvements following intervention implementation.
Assessment Framework
A structured checklist-based evaluation was developed based on best global practices in pediatric facility design, drawing from evidence-based design literature [1]Bock EP, Nilsson S, Jansson PA, et al. Literature review: evidence-based health outcomes and perceptions of the built environment in pediatric hospital facilities. J Pediatr Nurs. 2021;61:e42-e50. doi:10.1016/j.pedn.2021.04.013, [4]Bole A, Bernstein A, White MJ; Council on Environmental Health and Climate Change; Section on Minority Health, Equity, and Inclusion. The built environment and pediatric health. Pediatrics. 2024;153(1):e2023064772. doi:10.1542/peds.2023-064772 and pediatric engagement models [6]Gaminiesfahani H, Lozanovska M, Tucker R. A scoping review of the impact on children of the built environment design characteristics of healing spaces. HERD. 2020;13(4):98-114. doi:10.1177/1937586720903845, [7]Laursen J, Danielsen A, Rosenberg J. Effects of environmental design on patient outcome: a systematic review. HERD. 2014;7(4):108-119. doi:10.1177/193758671400700410. The audit tool was also informed by Joint Commission International (JCI) standards, particularly those related to patient safety, infection control, and emergency preparedness in pediatric care environments [16]Joint Commission International. (2024). Joint Commission International Accreditation Standards for Hospitals (8th ed.). Joint Commission International.. These global benchmarks were adapted for local applicability through a human-centered design lens, incorporating contextual relevance for LMIC settings. The HackPeds framework has been iteratively refined through repeat implementation in clinical audits, ensuring both rigor and adaptability in diverse pediatric healthcare environments.
The checklist covered multiple domains:
- Pediatric space design and engagement. Evaluated the presence of child-friendly infrastructure, play areas, interactive features, and accessibility.
- Safety and emergency preparedness. Assessed pediatric resuscitation readiness, infection control protocols, and emergency response procedures.
- Privacy and comfort. Examined the availability of breastfeeding areas, caregiver-friendly spaces, and patient privacy compliance.
- Parental engagement and education. Measured structured caregiver counseling, safety education programs, and feedback mechanisms.
- Emotional well-being and support. Evaluated the integration of storytelling interventions, play therapy, and other child-centered anxiety reduction techniques.
- Staff training and competency. Reviewed staff expertise in pediatric resuscitation (BLS, PALS, NRP), patient communication, and play therapy techniques.
- Process improvement and quality control. Examined CQI implementation, performance tracking mechanisms, and structured feedback loops for sustainability.
Structured Staff Interviews
Fifteen healthcare professionals participated in structured interviews designed to capture operational challenges and frontline insights. These included:
- Ten pediatric nurses and medical officers involved in direct pediatric inpatient and outpatient care.
- Five frontline staff from emergency and outpatient departments.
A standardized interview guide was used to ensure consistency across responses, minimizing variability and enhancing the reliability of qualitative insights. The primary interviewer (auditor), previously described, had extensive experience conducting interviews with on-ground staff in pediatric and other hospital units.
Interview responses were systematically categorized to identify recurring themes in pediatric care delivery. To mitigate potential bias, the EHL team was not involved in conducting the interviews.
The interview checklist was intended for use by a multidisciplinary team - including doctors, nurses, and technicians. Unit leads (e.g., senior doctor, nurse manager, unit manager) were encouraged to participate in the audit process, alongside the on-ground team. If interviews were conducted randomly, the on-call team was involved following the suggested approach.
A consensus-based approach was preferred during the interview process. In cases of inconsistencies or conflicts between responses from different team members, triangulation was applied. The presence of unit leads during this process was strongly recommended to help resolve discrepancies and ensure balanced insights. This approach also helped mitigate observer bias.
Facility Walkthroughs
A structured observational approach was used to assess spatial utilization, patient flow pathways, pediatric emergency preparedness, and caregiver engagement areas. Specific areas of evaluation included:
- Waiting areas, play zones, and interactive spaces for pediatric engagement.
- Pediatric emergency response readiness, resuscitation equipment placement, and staff response training.
- Caregiver engagement facilities, including breastfeeding stations and family support spaces.
To minimize observer bias, each assessment was independently documented before being triangulated with staff interviews and checklist-based findings. The EHL team provided support in coordinating walkthrough logistics but was not involved in direct observations or reporting.
PediTales: A Storytelling-Based Engagement Intervention
PediTales was implemented as a core intervention within HackPeds to enhance pediatric patient satisfaction and caregiver engagement through culturally tailored storytelling (paper in review). Designed as a bilingual (English and Urdu) initiative, PediTales leveraged interactive storytelling to create a more child-friendly hospital experience, particularly in the OPD and vaccination areas. The intervention aimed to reduce anxiety, improve health literacy, and strengthen patient-caregiver-provider relationships.
Implementation Strategy for PediTales
The intervention followed a structured Plan-Do-Study-Act (PDSA) cycle:
- Story development: Contextually relevant pediatric stories were created and adapted for a healthcare setting. The stories incorporated engaging visuals and simple, age-appropriate language.
- Staff training: Volunteers and pediatric staff received dynamic storytelling training, equipping them to engage children effectively.
- Pilot implementation: PediTales was introduced in the OPD and vaccination areas at Evercare Lahore, utilizing both digital (LCD screens, tablets) and printed materials.
- MoodBoard data collection: A visual analog scale (MoodBoard) was used to measure pediatric, caregiver, and staff engagement levels pre- and post-storytelling sessions.
- CQI and refinements: Feedback from MoodBoard responses was analyzed to iteratively refine the stories, improve training, and optimize integration into clinical workflows.
Benchmarking and Supporting Evidence
The HackPeds audit methodology was informed by global pediatric hospital design frameworks and previous research on child engagement, distraction-based storytelling interventions, and culturally relevant hospital-based pediatric innovations. This included:
- Health literacy and storytelling interventions shown to reduce pediatric distress and improve engagement [17]Norton-Westwood D, Pearson A, Robertson-Malt S. The ability of environmental healthcare design strategies to impact event-related anxiety in paediatric patients: a comprehensive systematic review. JBI Libr Syst Rev. 2011;9(44):1828-1882. doi:10.11124/01938924-201109440-00001, [8]Butt W, Mustafa F, Ahsan Z, Salim S, Tahir H, Mian A. The immunization questionnaire for understanding unwellness (TIQUU): fun learning about vaccination using an innovative storytelling approach. Vacunas (Engl Ed). 2024;25:304-312. doi:10.1016/j.vacune.2024.08.002, [9]Ahmad H, Naeem R, Feroze A, et al. Teaching children road safety through storybooks: an approach to child health literacy in Pakistan. BMC Pediatr. 2018;18(1):31. doi:10.1186/s12887-018-0982-5.
- Pediatric hospital innovation frameworks that enhance patient-centered care through structured quality improvement initiatives [10]Farooqi W, Subhani F, Mian A. Paediatric innovation in Pakistan: our experience and a call to action. Arch Dis Child. 2017;102(10):963-967. doi:10.1136/archdischild-2016-312123, [11]Madhani S, Farooqi WH, Mian AI. Stimulating innovation through the hackathon concept in paediatrics: our experience at the Aga Khan University. Arch Dis Child. 2017;102(10):994. doi:10.1136/archdischild-2017-313648.
- Evidence-based recommendations on pediatric hospital space optimization and caregiver inclusion in facility design [18]France DJ, Throop P, Walczyk B, et al. Does patient-centered design guarantee patient safety? Using human factors engineering to find a balance between provider and patient needs. J Patient Saf. 2005;1(3):145-153. doi:10.1097/01.jps.0000191550.92042.36.
Data Analysis
Quantitative data, including compliance rates, workflow efficiency metrics, and facility utilization statistics, were obtained from EHL’s IT specialists, electronic health records personnel, and patient safety teams. These performance indicators included:
- Patient flow times, triage categorization accuracy, and pediatric resuscitation preparedness.
- Space utilization trends before and after interventions.
- Staff competency improvements in pediatric engagement techniques.
Since the audit relied on hospital-reported indicators rather than independent data collection, analysis focused on trend identification and comparative evaluation across the baseline and re-audit phases. Additionally, qualitative insights from structured interviews were systematically analyzed for thematic patterns in pediatric care experience, facility engagement, and operational barriers.
Ethical Considerations
This audit was conducted as part of a hospital-led quality improvement initiative approved by EHL leadership, aligning with institutional patient safety and operational enhancement objectives. Since the study involved retrospective analysis of operational metrics without direct patient data collection, formal Institutional Review Board approval was not required. All evaluations adhered to ethical best practices for quality improvement research, ensuring confidentiality, transparency, and minimal disruption to hospital workflows.
RESULTS
A structured clinical audit was conducted at Evercare Hospital Lahore (EHL) in November 2024 to assess pediatric healthcare space design, safety, staff training, and caregiver engagement. The baseline audit revealed that pediatric spaces, particularly in the OPD and vaccination areas, were largely underutilized, lacking interactive engagement zones designed to reduce anxiety and improve patient experience. There was an absence of structured play areas, storytelling interventions, and child-friendly visual elements. The vaccination area, a high-traffic pediatric zone, was sterile and uninviting, contributing to heightened stress among children and caregivers. Additionally, inconsistencies in pediatric emergency preparedness were noted, with inadequate resuscitation equipment audits and limited staff training in pediatric-specific emergency response protocols. Parental engagement mechanisms were also absent, with no structured nutritional counseling, safety education, or caregiver feedback processes in place.
Table 1 presents the detailed findings from the baseline audit, capturing deficiencies across pediatric engagement spaces, safety protocols, caregiver education, and staff training.
Table 1: HackPeds: Key findings from the first audit (November 2024: Baseline)
Section | Key Element | Status | Observations | Recommendations |
|---|---|---|---|---|
Pediatric space design and engagement | Interactive play areas | Absent | No structured engagement spaces | Transform spaces into vibrant play and activity zones |
Pediatric space design and engagement | Underutilized spaces in OPD and IPD | Underutilized | Areas not optimized for pediatric engagement | Repurpose areas for play and learning activities |
Pediatric space design and engagement | Pediatric passage walls | Lacking | Walls lack visual appeal for children | Introduce colorful, interactive murals |
Safety and emergency preparedness | Pediatric emergency response measures | Inconsistent | No standardized response protocols in place | Introduce standardized pediatric rapid-response systems |
Safety and emergency preparedness | Resuscitation equipment maintenance | Irregular | Gaps in maintenance and readiness | Implement regular audits and maintenance schedules |
Privacy and comfort | Breastfeeding-friendly spaces | Limited | No designated private spaces | Design and introduce dedicated breastfeeding pods |
Parental engagement and education | Nutritional & safety counseling | Absent | No structured caregiver education programs | Implement structured counseling programs |
Parental engagement and education | Parental feedback mechanisms | Absent | No system to collect caregiver input | Establish structured feedback systems |
Emotional well-being and support | Storytelling in vaccination rooms | Absent | No engagement strategies during vaccinations | Introduce regular storytelling sessions |
Emotional well-being and support | Play therapy and emotional support training | Inconsistent | Staff not trained in structured play therapy | Develop staff training modules for emotional well-being |
Staff training and competency | Pediatric resuscitation training | Limited | Low completion rates for PALS/BLS | Implement mandatory training programs (BLS, PALS, etc.) |
Staff training and competency | Play therapy training | Inconsistent | Training programs not standardized | Develop structured play therapy training programs |
Process improvement and quality control | Structured satisfaction surveys | Absent | No mechanism to track patient/caregiver satisfaction | Establish regular caregiver and child satisfaction surveys |
Process improvement and quality control | CQI processes | Absent | No structured system for continuous improvement | Develop a CQI framework with regular reviews |
Interventions Implemented (November 2024 - January 2025)
Following the findings from the initial audit, a three-month intervention phase was undertaken to address the identified gaps. Key interventions included:
- Pediatric Engagement Spaces: Introduction of structured play areas in OPD waiting areas, incorporating age-appropriate toys, books, and interactive stations.
- Storytelling in Vaccination Rooms (PediTales): Pilot implementation of the PediTales program, a bilingual storytelling intervention aimed at reducing pediatric anxiety.
- Pediatric Emergency Preparedness: Standardization of rapid-response protocols for pediatric emergencies and initiation of routine equipment audits.
- Parental Engagement and Education: Launch of structured nutritional counseling and safety education sessions for caregivers.
- Staff Training and CQI Integration: Rollout of PALS/BLS training programs and formation of a CQI subcommittee to track intervention effectiveness.
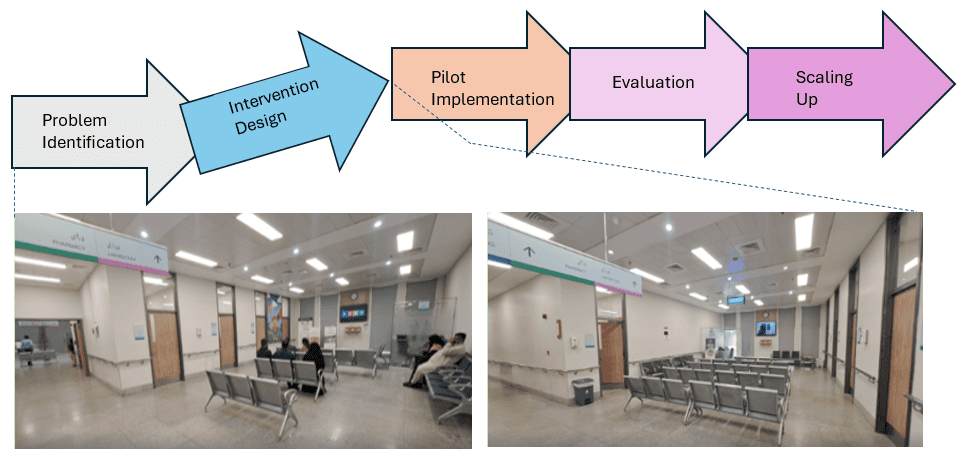
Figure 1: Pediatric Care Improvement Flow Diagram
Problem Identification
Pilot
Implementation
Evaluation
Scaling
Up
Intervention Design
Findings from the PediTales Pilot
PediTales was introduced as part of HackPeds to enhance child engagement and reduce hospital-related anxiety through immersive storytelling . The pilot was implemented in the OPD and vaccination areas at Evercare Lahore, integrating both digital (LCD screens, tablets) and printed storytelling materials.
MoodBoard Insights and Engagement Trends
MoodBoard responses collected from children, caregivers, and staff revealed promising trends:
- Children showed a 50% increase in positive engagement with healthcare teams after storytelling sessions.
- Caregivers reported feeling 40% more reassured, citing a more welcoming and child-friendly hospital environment.
- Staff noted improved interactions with pediatric patients, recognizing storytelling as an effective tool for anxiety reduction.
However, initial findings indicated that structured workflow integration remained a challenge. Some staff required additional training in dynamic storytelling techniques, and ongoing feedback loops were necessary to refine the stories for maximum impact. Table 2 summarizes the key findings from the re-audit, capturing measurable progress and areas requiring further refinement.
Table 2: HackPeds: Re-audit findings (January 2025, after targeted interventions)
Section | Key Element | Status | Observations | Quarterly Update Metrics |
|---|---|---|---|---|
Pediatric space design and engagement | Interactive play areas | Pilot phase | Play spaces implemented in OPD | Number of child-friendly zones created |
Pediatric space design and engagement | Pediatric passage walls | In progress | Murals and interactive storytelling areas added | Parent/staff feedback survey results |
Safety and emergency preparedness | Pediatric emergency response measures | Improved | Standardized rapid-response protocol introduced | Compliance with pediatric emergency drills |
Safety and emergency preparedness | Resuscitation equipment maintenance | Partially implemented | Some gaps remain in audit frequency | Percentage of equipment audited quarterly |
Privacy and comfort | Breastfeeding-friendly spaces | Limited improvement | Some pods introduced, but accessibility issues remain | Usage frequency of breastfeeding areas |
Parental engagement and education | Nutritional & safety counseling | Pilot phase | Initial sessions held, but limited caregiver attendance | Number of counseling sessions conducted |
Parental engagement and education | Parental feedback mechanisms | Launched | Structured caregiver feedback surveys implemented | % of caregivers surveyed |
Emotional well-being and support | Storytelling in vaccination rooms (PediTales) | Pilot phase | Bilingual storytelling introduced | MoodBoard engagement ratings |
Emotional well-being and support | Play therapy and emotional support training | Ongoing | Training modules rolled out, but participation gaps remain | Number of trained staff |
Staff training and competency | Pediatric resuscitation training | Inconsistent | Some training programs conducted, but compliance remains low | % of staff certified quarterly |
Staff training and competency | Play therapy training | Limited | Training programs initiated, but need refinement | % of staff completing play therapy training |
Process improvement and quality control | Structured satisfaction surveys | Established | CQI committee formed and tracking in place | KPI review frequency |
Process improvement and quality control | CQI processes | Ongoing | Initial data tracking implemented | % of improvement initiatives successfully completed |
Scalability and Projected Outcomes
The audit results underscore the scalability of HackPeds interventions in pediatric healthcare settings, with measurable improvements in pediatric engagement, emergency preparedness, and parental participation. The introduction of structured play areas, interactive storytelling sessions (PediTales), and caregiver education initiatives demonstrated tangible benefits in reducing child anxiety, enhancing caregiver experience, and improving staff-patient interaction dynamics.
However, certain operational challenges persist. While PediTales was well received, its structured integration into routine workflows remains a work in progress. Similarly, staff participation in play therapy and resuscitation training increased but remains below optimal compliance levels. The re-audit also highlighted gaps in sustained caregiver engagement, necessitating ongoing refinement of feedback loops and educational programming.
As shown in Table 2, the incorporation of CQI tracking mechanisms allowed for iterative adjustments in interventions, reinforcing the value of continuous quality monitoring over static, one-time implementations. If further refinements are made, projected outcomes include:
- 25–35% increase in pediatric engagement and interactive play area utilization,
- Improvements in structured caregiver education session attendance,
- Higher compliance rates in pediatric emergency response training,
- Expanded storytelling interventions with refined bilingual models.
Future audits in Nigeria and Kenya will evaluate whether these improvements can be replicated across diverse pediatric hospital environments, further validating the scalability of HackPeds interventions.
DISCUSSION
The HackPeds audit identified systemic gaps in pediatric space design, safety protocols, and caregiver engagement, reinforcing the need for structured, child-friendly interventions. The findings revealed underutilized play areas, inconsistencies in pediatric emergency preparedness, limited privacy for breastfeeding mothers, and insufficient parental and staff engagement mechanisms. Addressing these gaps through targeted interventions has the potential to significantly enhance pediatric care experiences, aligning with global best practices and reinforcing a patient-centered approach.
One of the most notable strengths of this audit was its ability to systematically assess pediatric healthcare environments through a structured, evidence-based methodology. Unlike traditional assessments that often rely on anecdotal insights, HackPeds provided quantifiable data on both baseline deficiencies and post-intervention improvements. By incorporating structured play spaces, storytelling interventions, and caregiver engagement mechanisms, the audit demonstrated tangible progress in transforming the pediatric care experience at Evercare Hospital Lahore (EHL). The iterative audit approach also allowed for adaptive refinements, reinforcing HackPeds’ capacity as a replicable and scalable CQI framework.
The absence of interactive play spaces and storytelling interventions emerged as a key barrier to pediatric engagement, a finding consistent with prior research indicating that structured play and storytelling can reduce pediatric anxiety and enhance cooperation during medical procedures [1]Bock EP, Nilsson S, Jansson PA, et al. Literature review: evidence-based health outcomes and perceptions of the built environment in pediatric hospital facilities. J Pediatr Nurs. 2021;61:e42-e50. doi:10.1016/j.pedn.2021.04.013, [2]Cartland J, Ruch-Ross HS, Carr L, et al. The role of hospital design in reducing anxiety for pediatric patients. HERD. 2018;11(3):66-79. doi:10.1177/1937586718779219. The implementation of PediTales at EHL represents an innovative adaptation of these concepts, integrating AI-powered, culturally tailored storytelling into pediatric care. Preliminary findings from the MoodBoard assessment suggest increased child engagement and parental confidence, yet the initiative remains in an early phase, requiring further integration into clinical workflows for sustained impact.
Beyond engagement, the audit underscored systemic inconsistencies in pediatric emergency preparedness, highlighting gaps in staff training, resuscitation equipment audits, and emergency response protocols. These findings align with global studies emphasizing the critical role of structured pediatric resuscitation programs, including BLS and PALS certification [3]Phuria S. The role of hospital design in improving patient recovery. Int J Adv Res. 2024;12:670-675. doi:10.21474/IJAR01/19499. While the introduction of standardized training led to modest improvements, compliance rates remained suboptimal, signaling the need for ongoing reinforcement. HackPeds’ structured CQI approach, however, enabled the hospital to track incremental improvements over time, demonstrating its capacity to drive long-term enhancements in emergency preparedness.
Parental engagement and health literacy also emerged as critical areas for intervention. Research has consistently demonstrated that structured parental counseling, real-time feedback mechanisms, and health literacy tools enhance caregiver confidence and adherence to treatment plans [4]Bole A, Bernstein A, White MJ; Council on Environmental Health and Climate Change; Section on Minority Health, Equity, and Inclusion. The built environment and pediatric health. Pediatrics. 2024;153(1):e2023064772. doi:10.1542/peds.2023-064772. The integration of bilingual health literacy resources and structured parental education programs through PediTales offers a promising pathway for addressing these deficiencies. By integrating structured pediatric engagement mechanisms, HackPeds not only improved child and caregiver satisfaction but also demonstrated operational benefits. Prior studies suggest that patient-centered design approaches can enhance provider efficiency and streamline workflow, reinforcing the need for scalable pediatric quality improvement frameworks [19]Brown KK, Gallant D. Impacting patient outcomes through design: acuity adaptable care/universal room design. Crit Care Nurs Q. 2006;29(4):326-341. doi:10.1097/00002727-200610000-00006. However, the audit also revealed that caregiver participation remained inconsistent, highlighting the need for additional efforts to promote sustained parental involvement in pediatric care.
One of the most important contributions of this audit was the validation of HackPeds as a CQI model. The structured baseline assessment, intervention phase, and re-audit process allowed for the quantification and qualification of post-implementation improvements. Unlike static quality improvement efforts, HackPeds functioned as a dynamic, iterative model, continuously refining its interventions based on real-time data. The ability to track measurable improvements in pediatric engagement, emergency preparedness, and caregiver participation underscores HackPeds’ potential as a scalable and adaptable framework for hospital-wide pediatric quality enhancement. Similar flexible hospital design models, such as acuity-adaptable care, have been shown to improve patient-centered outcomes and operational efficiency [20]Swingler G, Hendricks M, Hall D, et al. Can a new paediatric sub-specialty improve child health in South Africa? S Afr Med J. 2012;102(9):738-739. Accessed March 24, 2025. https://www.ajol.info/index.php/samj/article/view/80826.
Despite these strengths, several limitations of the audit must be acknowledged. The one-day audit conducted by a single auditor may have restricted the depth of findings, particularly in assessing long-term operational challenges. However, the process has already undergone further validation through re-audits at EHL’s pediatric spaces in January 2025, expanding beyond the initial November 2024 audit. In addition, other unit-specific audits (ICUs, emergency department, etc.) have also been conducted in November 2024 and January 2025. Iterations of the unit-based checklists have been tested in Lagos, Nigeria in March 2025 (data review ongoing). Additionally, future audits are planned in Kenya. This iterative multi-site validation approach strengthens the framework’s reliability. A CQI model is now integrated into this process, ensuring that audits are not static but continuously monitored, refined, and reinforced with measurable impact.
Another limitation was that the number of pediatric patients present during the audit was not systematically recorded, limiting the ability to derive comprehensive patient-centered insights. While global literature suggests similar improvements in patient satisfaction following pediatric-friendly interventions, our estimate of a 30–40% projected improvement is based on preliminary observations, caregiver feedback, and staff discussions. However, site-specific pre/post satisfaction metrics were not systematically collected at Evercare, limiting direct comparative analysis. Future assessments should incorporate structured patient-reported outcome measures to validate these projections.
A key consideration in the scalability of HackPeds interventions is resource feasibility. Many LMIC hospitals operate with limited budgets, making large-scale infrastructure modifications challenging. However, HackPeds demonstrated that low-cost, high-impact interventions such as murals, interactive storytelling, and structured caregiver education programs can be implemented with minimal financial burden. These interventions serve as an entry point for more comprehensive pediatric care improvements while remaining adaptable to different institutional capacities.
The relevance of HackPeds extends beyond Evercare Lahore. Similar pediatric engagement and CQI models have been successfully implemented in LMIC settings, such as the child-friendly outpatient redesigns in South African district hospitals [21]Swingler G, Hendricks M, Hall D, et al. Can a new paediatric sub-specialty improve child health in South Africa? S Afr Med J. 2012;102(9):738-739. Accessed March 24, 2025. https://www.ajol.info/index.php/samj/article/view/80826 and structured play therapy programs in Indian pediatric wards [22]Raman V, Singhal M. Play therapy with children: its relevance and utility in the Indian context. J Indian Assoc Child Adolesc Ment Health. 2015;11:121-157. doi:10.1177/0973134220150203. These examples reinforce HackPeds’ viability as a scalable intervention, particularly in resource-constrained environments where structured, data-driven pediatric quality improvement frameworks are often lacking.
To address the identified limitations, a series of follow-up audits and process improvements have been outlined. Expanded audits at Evercare Hospitals in Lahore and Lekki in 2025 will extend the scope to include ICUs, emergency departments, and other units. Multi-site validation in Nigeria and Kenya will assess HackPeds’ applicability across different healthcare environments. Further refinement of PediTales will focus on optimizing cultural adaptability and workflow integration, while structured caregiver feedback mechanisms will enhance parental engagement strategies. Additionally, the development of a pediatric innovation analytics dashboard will strengthen CQI mechanisms, providing real-time tracking of intervention effectiveness.
Conclusion
The HackPeds audit highlights the potential for structured, scalable interventions to improve pediatric healthcare environments. By addressing gaps in pediatric engagement, safety, and caregiver education, HackPeds provides a framework for sustainable, patient-centered improvements. The integration of interactive play spaces, privacy enhancements, structured staff training programs, and storytelling-based patient engagement strategies will be critical in transforming pediatric healthcare spaces into environments that are safer, more engaging, and operationally efficient. Future audits will play a pivotal role in assessing the replicability of these interventions across diverse healthcare settings, further reinforcing HackPeds as a scalable model for pediatric hospital transformation.
Disclosure and Funding Statement: This research received no external funding from any public, private, or commercial entity. Dr. Asad Mian and Mr. Taha Anver are co-founders of Innovly, a startup focused on innovation-driven healthcare solutions. The clinical audit framework utilized in this study was developed and previously validated by Innovly; however, no financial compensation was received by Innovly for this endeavor, and its use in this research was solely for quality improvement and validation purposes.
Acknowledgment Statement: The authors extend their gratitude to all pediatrics departments that participated in HackPeds audits, whose insights helped refine the framework. We also sincerely appreciate the doctors, nurses, administrators, and staff at Evercare Hospital Lahore for their openness, availability, and collaboration throughout the audit process.
REFERENCE LIST
- Bock EP, Nilsson S, Jansson PA, et al. Literature review: evidence-based health outcomes and perceptions of the built environment in pediatric hospital facilities. J Pediatr Nurs. 2021;61:e42-e50. doi:10.1016/j.pedn.2021.04.013
- Cartland J, Ruch-Ross HS, Carr L, et al. The role of hospital design in reducing anxiety for pediatric patients. HERD. 2018;11(3):66-79. doi:10.1177/1937586718779219
- Phuria S. The role of hospital design in improving patient recovery. Int J Adv Res. 2024;12:670-675. doi:10.21474/IJAR01/19499
- Bole A, Bernstein A, White MJ; Council on Environmental Health and Climate Change; Section on Minority Health, Equity, and Inclusion. The built environment and pediatric health. Pediatrics. 2024;153(1):e2023064772. doi:10.1542/peds.2023-064772
- Watts R, Wilson S. Impact of the physical environment in paediatric hospitals on health outcomes: a systematic review. JBI Libr Syst Rev. 2009;7(20):908-941. doi:10.11124/01938924-200907200-00001
- Gaminiesfahani H, Lozanovska M, Tucker R. A scoping review of the impact on children of the built environment design characteristics of healing spaces. HERD. 2020;13(4):98-114. doi:10.1177/1937586720903845
- Laursen J, Danielsen A, Rosenberg J. Effects of environmental design on patient outcome: a systematic review. HERD. 2014;7(4):108-119. doi:10.1177/193758671400700410
- Butt W, Mustafa F, Ahsan Z, Salim S, Tahir H, Mian A. The immunization questionnaire for understanding unwellness (TIQUU): fun learning about vaccination using an innovative storytelling approach. Vacunas (Engl Ed). 2024;25:304-312. doi:10.1016/j.vacune.2024.08.002
- Ahmad H, Naeem R, Feroze A, et al. Teaching children road safety through storybooks: an approach to child health literacy in Pakistan. BMC Pediatr. 2018;18(1):31. doi:10.1186/s12887-018-0982-5
- Farooqi W, Subhani F, Mian A. Paediatric innovation in Pakistan: our experience and a call to action. Arch Dis Child. 2017;102(10):963-967. doi:10.1136/archdischild-2016-312123
- Madhani S, Farooqi WH, Mian AI. Stimulating innovation through the hackathon concept in paediatrics: our experience at the Aga Khan University. Arch Dis Child. 2017;102(10):994. doi:10.1136/archdischild-2017-313648
- Bhimani S, Brown N, Mian AI. Streamlining pediatric emergency medicine at a tertiary-care hospital of a low- to middle-income country. Indian Pediatr. 2015;52:1021-1024. Accessed March 24, 2025. https://indianpediatrics.net/dec2015/dec-1021-1024.htm
- Innovly. (2025, March 11). Innovly: Healthcare innovation platform. https://innovly.net/
- Evercare Group. (2025, March 11). Evercare Group: Transforming healthcare. https://www.evercaregroup.com/
- Evercare Hospital Lahore. (2025, March 11). Evercare Hospital Lahore. https://www.evercarehospitallahore.com/
- Joint Commission International. (2024). Joint Commission International Accreditation Standards for Hospitals (8th ed.). Joint Commission International.
- Mian A. The power of the uncarved block and the need to be childlike now more than ever. The Express Tribune. June 12, 2022. Accessed March 24, 2025. https://tribune.com.pk/story/2361088/the-power-of-the-uncarved-block-and-the-need-to-be-childlike-now-more-than-ever
- Norton-Westwood D, Pearson A, Robertson-Malt S. The ability of environmental healthcare design strategies to impact event-related anxiety in paediatric patients: a comprehensive systematic review. JBI Libr Syst Rev. 2011;9(44):1828-1882. doi:10.11124/01938924-201109440-00001
- France DJ, Throop P, Walczyk B, et al. Does patient-centered design guarantee patient safety? Using human factors engineering to find a balance between provider and patient needs. J Patient Saf. 2005;1(3):145-153. doi:10.1097/01.jps.0000191550.92042.36
- Brown KK, Gallant D. Impacting patient outcomes through design: acuity adaptable care/universal room design. Crit Care Nurs Q. 2006;29(4):326-341. doi:10.1097/00002727-200610000-00006
- Swingler G, Hendricks M, Hall D, et al. Can a new paediatric sub-specialty improve child health in South Africa? S Afr Med J. 2012;102(9):738-739. Accessed March 24, 2025. https://www.ajol.info/index.php/samj/article/view/80826
- Raman V, Singhal M. Play therapy with children: its relevance and utility in the Indian context. J Indian Assoc Child Adolesc Ment Health. 2015;11:121-157. doi:10.1177/0973134220150203
Declarations
Ethics approval and consent to participate
The manuscript reports that this hospital-led quality improvement audit did not require formal Institutional Review Board approval because it used retrospective operational metrics without direct patient data collection.
Consent for publication
Not applicable.
Availability of data and materials
The pediatric healthcare-space audit data are not publicly available because they relate to internal hospital quality improvement operations. De-identified summary materials may be available from the corresponding author on reasonable request, subject to institutional approval.
Authors' contributions
Asad I Mian: Writing - original draft; Conceptualization; Investigation; Methodology; Data curation | Muhammad Taha Anver: Writing - review and editing | Mahreen Sulaiman: Writing - review and editing | Zunaira Namal: Writing - review and editing | Kazim Ali Tarar: Writing - review and editing | Ayoola Shonibare: Writing - review and editing | Irfan Khan: Writing - review and editing
Competing interests
No conflict of interest was disclosed in onboarding data or article text.
Funding
No funding was disclosed in onboarding data or article text.