

Abstract
Background: Healthcare systems in low- and middle-income countries [LMICs] face systemic challenges in high-stakes environments such as emergency medicine and intensive care. Limited resources, fragmented workflows, and communication gaps often compromise patient care. Human-Centered Design Thinking [HCDT] provides an empathy-driven, iterative framework for problem-solving tailored to these settings.
Methods: Two HCDT workshops were conducted in 2024 at Evercare hospitals in Lekki [Nigeria] and Lahore [Pakistan]. Using the Stanford d.school’s five-step framework—Empathy, Problem Definition, Ideation, Prototyping, and Testing—participants applied tools including empathy mapping, PICO problem dissection, brainstorming, and rapid prototyping. Teams included physicians, nurses, paramedics, and administrators.
Results: Eighty-six participants engaged, with 23 structured evaluations per site. In Lekki, solutions addressed referral delays and communication gaps through referral coordinators, checklists, and digital tools. In Lahore, ICU-focused teams developed interventions for staff turnover, communication inefficiencies, and humanization of care—culminating in the Empatheon program, which applied PDSA cycles to strengthen staff well-being and patient-family engagement. Both sites reported high satisfaction, with >65% rating inspiration, knowledge, and practicality as very high.
Conclusion: HCDT shows strong potential to address healthcare challenges in LMICs through low-cost, scalable, and context-sensitive innovations. Embedding empathy, co-creation, and iteration into care processes enhances outcomes and fosters sustainable, patient-centered innovation. Further validation through real-world implementation is warranted.
Keywords: Human-Centered Design Thinking, healthcare innovation, LMICs, emergency medicine, critical care
Background/Rationale/Purpose
Healthcare systems in LMICs face unique systemic challenges, particularly in high-stakes areas like Emergency Medicine [EM] and Intensive Care Units [ICUs] [5]. Resource limitations, fragmented workflows, and communication gaps exacerbate inefficiencies, compromising patient care and operational outcomes. These challenges necessitate innovative approaches tailored to address the specific needs of critical care environments.
[2]Dam, R. F. (2023). The 5 Stages in the Design Thinking Process. Interaction Design Foundation., [9]IDEO. (2024). What’s the difference between human-centered design and design thinking? IDEO. Human-Centered Design Thinking [HCDT] offers a transformative methodology to tackle such issues by prioritizing empathy, collaboration, and iterative problem-solving. By aligning systemic improvements [3]Saeed, N., Sulaiman, M., & Mian, A. I. (2023). Human-Centered Design Thinking in the Emergency Department: Channeling the Chaos Together., [11]Villanova University. (2025). The power of human-centered design thinking in innovation., [12]Innovation & Entrepreneurship. Comparing human-centered design thinking with traditional problem-solving approaches. Innov Entrep. 2023;12:Article 291. with the needs of patients, families, and care teams, HCDT can enhance both clinical outcomes and operational efficiency.
In this context, HCDT workshops were conducted in 2024 at Evercare hospitals [3]Saeed, N., Sulaiman, M., & Mian, A. I. (2023). Human-Centered Design Thinking in the Emergency Department: Channeling the Chaos Together., [8]Innovation & Entrepreneurship. (2023). Comparing human-centered design thinking with traditional problem-solving approaches. in Lekki, Lagos, Nigeria, and Lahore, Pakistan, focusing on exploration of the application of HCDT in Lower Middle Income Countries [LMIC] to identify critical issues and develop solutions for emergency and intensive care management.
Objectives
The workshops aimed to:
- Identify critical pain points within emergency and intensive care operations, including specific units such as the Emergency Department, PICU, NICU, MICU, SICU, CCU, and Special Care Units.
- Co-create actionable solutions through multidisciplinary collaboration among participants from diverse professional backgrounds.
- Foster a culture of empathy-driven innovation to enhance patient care, team dynamics, and operational efficiency.
- Empower participants to integrate design thinking principles into their daily workflows, encouraging sustainable and innovative practices.
Methodology
The workshops employed Stanford d.school’s five-step HCDT framework [2]Dam, R. F. (2023). The 5 Stages in the Design Thinking Process. Interaction Design Foundation.: Empathy, Problem Definition, Ideation, Prototyping, and Testing (see Fig. 1). Each step was implemented in a structured manner, as listed below briefly.
- During the Empathy phase, participants reflected on patient and staff interactions to create detailed empathy maps.
- Problem Definition sessions used the PICO framework [1]Mian, A. I. (2021). #C2i-Create-2-Innovate. to dissect identified challenges, encouraging participants to craft "how might we" questions. PICO is a structured problem-dissection tool designed to guide teams in identifying and analyzing challenges by breaking them into four key components: Problem/Population [P] to define the issue and those affected, Ideation [I] to explore why the problem exists and its underlying causes, Context [C] to understand its relevance to local or global settings, and Outcome [O] to define the desired impact, feasibility, and sustainability of potential solutions.
- The Ideation phase involved brainstorming sessions using divergent and convergent thinking techniques to generate and refine solutions.
- Prototyping activities encouraged participants to create tangible models, such as digital tools or workflow processes.
- The Testing phase involved conceptualizing success metrics and feedback loops for real-world application [6]Kelley, T. (2016). The Art of Innovation: Lessons in Creativity from IDEO. Profile Books..
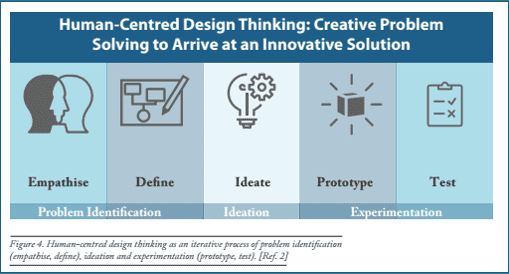
Figure 1. Evercare Group 2.0 workshops on HCDT as a 5-step process (see text for details).
Workshop Structure (Operations and format shown in Table 1 below as an example)
- The workshops, conducted at Lekki and Lahore in January and April of 2024, respectively, were between two to two and a half days long.
- They were designed to be contextually relevant for LMIC settings, emphasizing low-cost, scalable, and inclusive approaches to foster innovative problem-solving.
- Activities included empathy mapping, assumption-storming, PICO-guided problem dissection, and collaborative brainstorming.
- Facilitators used a mix of lectures, role-playing, and hands-on problem-solving exercises.
- All sessions were led by Evercare-based co-facilitators under the supervision and support of Prof. Dr. Asad Mian (AM) (senior author) as team lead.
Date | Module | Details/Activities | Facilitator(s) |
01/25/24 | Introduction | Introduction to HCDT: discuss need for complex problem solving; hack process | Asad Mian (AM) |
01/25/24 | Five steps of design thinking | Pre-thinking exercise: Break the ice; Recap HCDT in small groups; choose a specific topic within the theme to be hacked; E.g.: I would like to work on XYZ Assumption-storm: Pen down assumptions on a paper regarding the selected topic | AM/team |
Step I: Empathy | Looking through the lens of empathy: Participants will:
| AM/team | |
Step II: Problem Identification and Dissection | State the problem: Ask participants to write a problem statement, followed by a brief intro to PICO guidelines for problem dissection.
| AM/team | |
01/26/24 | Step III: Ideation | Low hanging fruit ideas to moonshots: Process of divergent and convergent thinking; ask participants to:
| AM/team |
time permitting | Step IV: Prototyping | Embrace experimentation Ask participants to:
| AM/team |
time permitting | Step V: Testing | Testing: Reflect on testing ; think of a testing paradigm for their favorite solution identified | AM/team |
Table 1. Schedule breakdown for the HCDT workshop at Lekki, Lagos, Nigeria. Total time ~ 5 hours over 2 days.
- Participants represented diverse professional roles, including clinicians, paramedics, nurses, and administrators, ensuring multidisciplinary collaboration throughout the workshops.
- Evaluations were collected from the participants at the end of each workshop.
- True to the low-cost and low fidelity nature of HCDT, other than PowerPoint/projection, laptops, Wi-Fi, the requirement was to be non-judgmental and non-hierarchical.
- This structured methodology empowered participants to generate actionable, context-specific solutions for critical care challenges [6]Kelley, T. (2016). The Art of Innovation: Lessons in Creativity from IDEO. Profile Books..
The outcomes of these workshops, including the innovative prototypes and their potential impact, are detailed in the following sections.
Results
Participant Demographics: A total of 41 participants attended the sessions in Lekki, and 45 in Lahore, with completed evaluations from 23 participants at each site. The majority of respondents were aged 31-40 years (52.2% in Lekki and 56.5% in Lahore), with a slightly higher proportion of males at both locations.
Key Findings
- Lekki (Emergency and Acute Care):
- Pain Points: Inefficient referrals, delayed emergency responses, and fragmented communication.
- Solutions: Referral coordinators, standardized checklists, and digital tools for communication.
- Metrics: Potential to reduce delays and improve patient satisfaction.
- Lahore (ICU Management):
- Pain Points: Delayed triage protocols and lack of empathy in patient care.
- Solutions: Empathy training leading to the establishment of Empatheon and revised triage protocols [7]Thiel, P. (2014). From Zero to One: Notes on Startups, or How to Build the Future. Crown Currency..
- Metrics: Improved staff confidence, triage accuracy, and patient satisfaction [4]Salim, Y. (2024). Healthcare Innovation Powered by AI. The Express Tribune..
Satisfaction Levels
Lekki
The HCDT workshop in Lekki demonstrated high participant satisfaction, as illustrated in the Educational Value and Logistical Factors graphs in Fig. 2A & B. Most participants rated inspiration (65% giving a score of 5) and knowledge enhancement (57% rating 5) very positively. The practicality of solutions also stood out, with 65% rating it 5. Team diversity and plans for further development were similarly well-rated, with the majority assigning scores of 4 or 5. For logistical factors, the workshop's relaxed and fun atmosphere received overwhelmingly positive ratings (74% scoring 5). However, adequacy of time received slightly more mixed feedback, with 43% rating it 5 and 35% rating it 4.
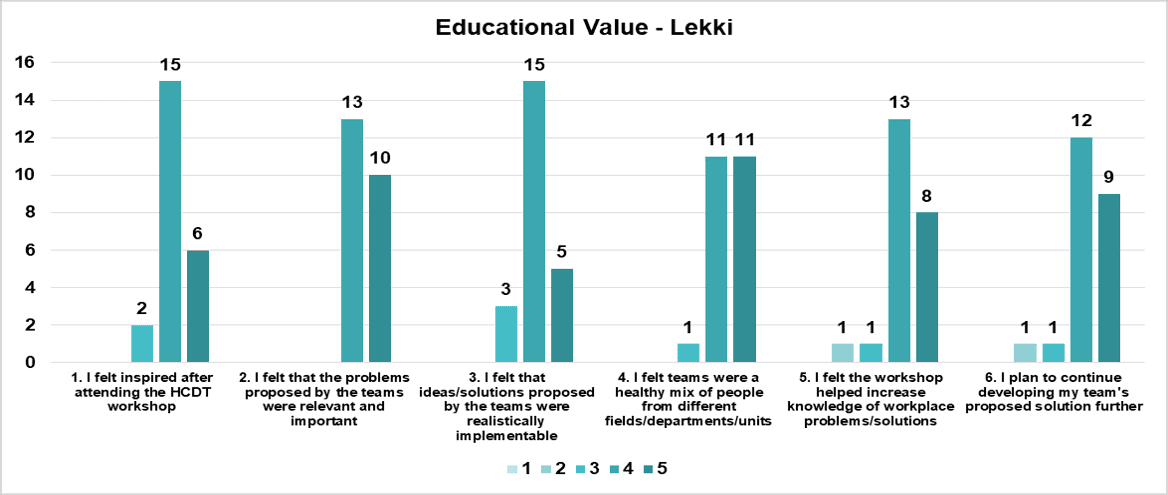
Figure 2A. Likert score distributions for Education Value for the HCDT workshop at Lekki, Jan 2024.
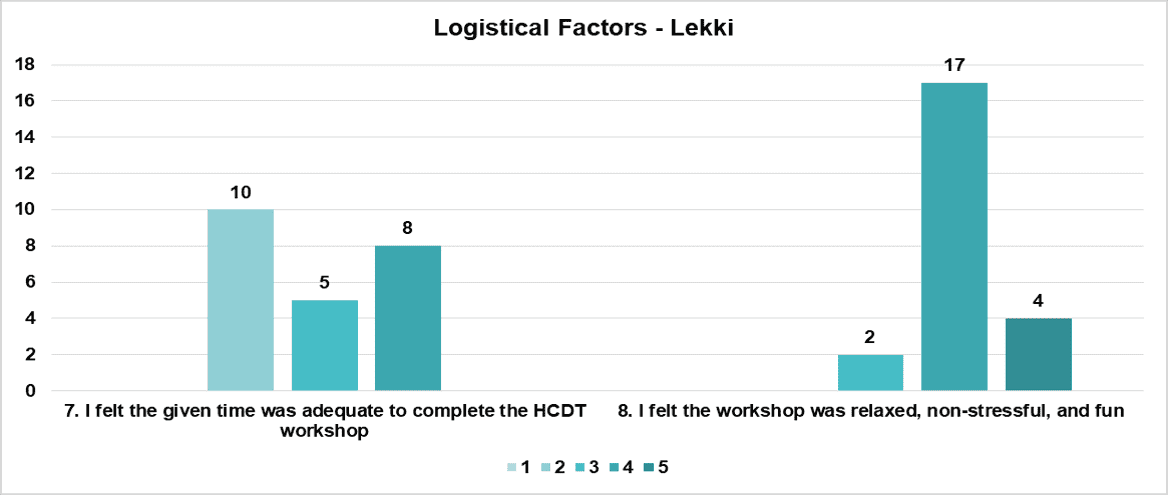
Figure 2B. Likert score distributions for Logistical Factors for the HCDT workshop at Lekki, Jan 2024.
Lahore
The HCDT workshop in Lahore also received strong feedback, as seen in the Educational Value and Logistical Factors graphs in Fig. 3A & B. Inspiration and knowledge enhancement were highly rated, with 70% of participants giving a score of 5 for each. Confidence in the practicality of solutions and team diversity were also notable, with the majority assigning ratings of 4 or 5. For logistical factors, while time adequacy received mixed ratings (43% rating 5, 39% rating 4), the relaxed and enjoyable workshop atmosphere was a highlight, with 57% scoring it 5.
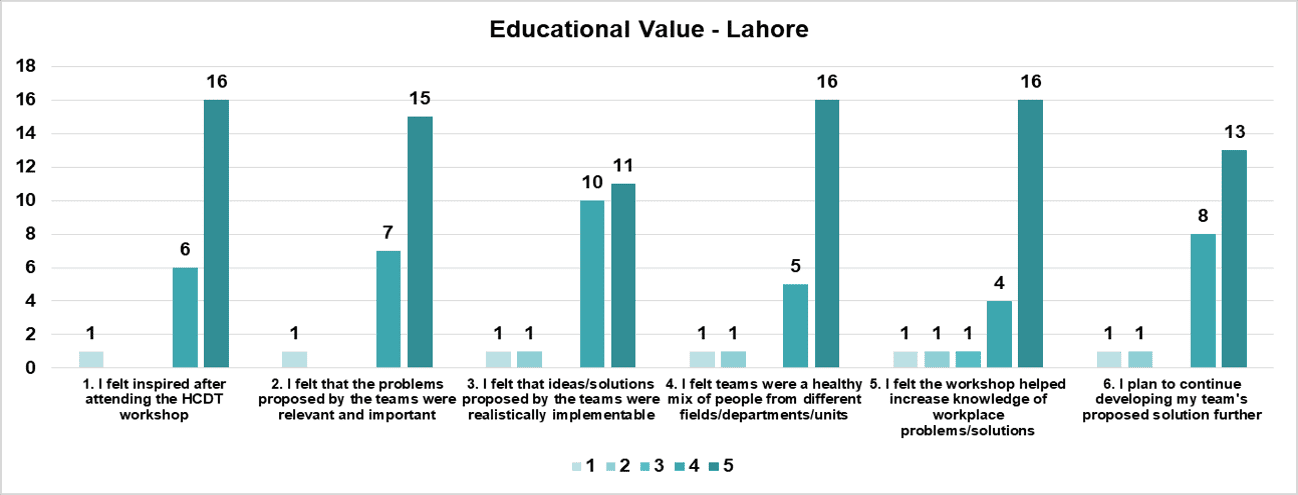
Figure 3A. Likert score distributions for Education Value for the HCDT workshop at Lahore, April 2024.
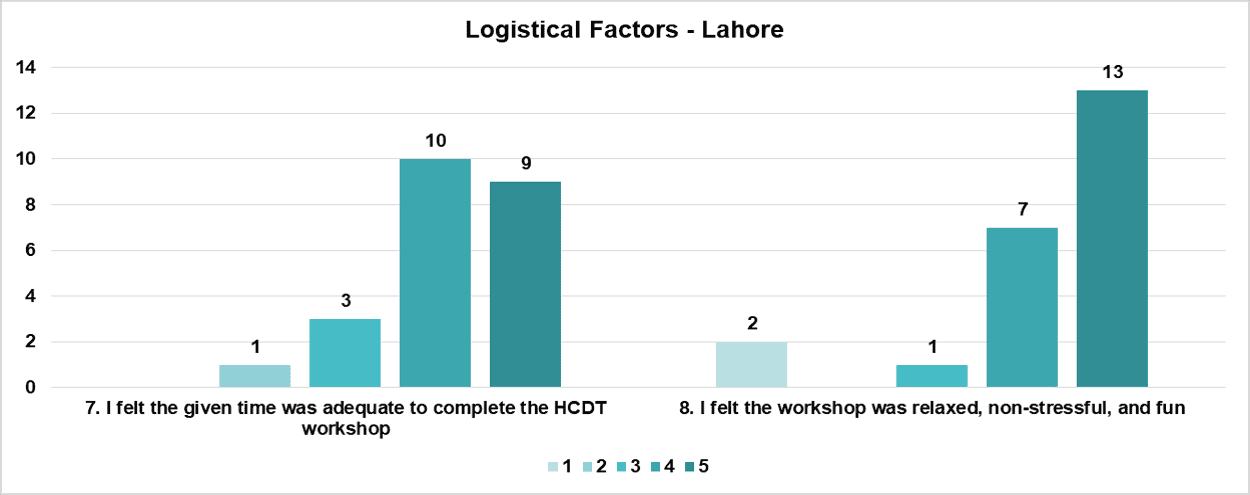
Figure 3B. Likert score distributions for Logistical Factors for the HCDT workshop at Lahore, April 2024.

Fig 4. Participant brainstorming sessions, role-playing activities, and empathy-mapping exercises demonstrate the high level of engagement and collaboration throughout the workshops (shown here for Lekki, Nigeria).
Post HCDT Incubation: Lekki, Lagos, Nigeria
Four teams—DEC-I, ERA, TalkLine, and Communications Hub—developed targeted prototypes addressing key challenges in emergency medicine, including referral inefficiencies, emergency response delays, and communication gaps among interdisciplinary teams (see Table 2). Prototypes developed as a result of focused group discussions, converging ideas derived from the brain storming session to one idea, by incorporating resource limitations, included sketches, models and initial frameworks of the proposed solutions. Prototypes ranged from referral pathways and pre-ED care improvements to communication training programs tailored to acute care and paramedic operations. While the teams advanced to the prototyping phase, no real-world testing has been conducted yet.
Team/Startup Name | Team Composition | Empathy/Pain Point/Problem Statement | Ideation (Convergent Thinking) | Prototyping Stage |
|---|---|---|---|---|
DEC-I (Referral System Improvement) | 11 members (paramedic, nurses, admin, orthopedic technician, etc.) | Poor referral system causing delays, miscommunication, staff burnout, and increased morbidity/mortality. | Policies/protocols, referral coordinator role, and centralized referral platform. | Focus on ED policies; paper-based solutions; metrics like reduced wait times and improved satisfaction. |
ERA (Emergency Response Enhancement) | 9 members (paramedics, intensivist, medical administrator, nurse, etc.) | Emergency response delays affecting patients, staff, Evercare reputation, and economic productivity. | Training/retraining emergency response team on communication and empathy. | Focus on paramedics and pre-ED care; develop training; measure reduced response times and patient feedback. |
TalkLine (Communication Improvement) | 11 members (ED staff, ICU staff, OBGYN, dialysis, business development, etc.) | Communication gaps among caregivers and with patients, leading to poor satisfaction and patient experience. | Workshops on communication, feedback template use, and conflict resolution. | Training on communication practices; conflict resolution; feedback mechanisms integrated into processes. |
Communications Hub (Communication Improvement) | 10 members (physiotherapists, medical officers, admin, interns, radiographers, etc.) | Poor interdisciplinary staff communication impacting operations and patient experience. | Training on communication ethics, respect, and task documentation. | Merge with TalkLine; focus on communication ethics; use feedback mechanisms and reflective practices. |
Table 2. Lekki, Nigeria: Summary of each team's composition, problem focus, and proposed solutions.
Post-HCDT Incubation: Lahore, Pakistan
The HCDT workshop in Lahore resulted in the formation of five teams focused on addressing challenges in ICUs and Critical Care Medicine, including staff turnover, communication gaps, and humanizing care. While there were five teams in total, detailed information could only be curated for three teams (see Table 3): Health Heroes, SHAFAA, and Empathy Listeners. These teams developed innovative solutions addressing critical issues such as improving staff well-being, enhancing communication in high-stakes ICU environments, and creating compassionate care models. Their prototypes reflect a commitment to improving outcomes in critical care settings, aligning with Evercare’s mission of patient-centered excellence.
Team/Startup Name | Team Composition | Empathy/Pain Point/Problem Statement | Ideation (Convergent Thinking) | Prototyping Stage |
|---|---|---|---|---|
Health Heroes (ICU Staff Turnover Reduction) | 5 members (nurses, ICU physicians, admin, patient experience staff) | High nurse turnover in a 30-bed ICU, leading to reduced care quality, staff burnout, and recruitment costs. | Flexible scheduling, wellness programs, recognition and rewards, and professional development. | Tested shift options, wellness events, recognition initiatives, and training programs; feedback loops to refine prototypes. |
SHAFAA (ICU Communication Improvement) | 4 members (ICU nurses, admin, communication specialists) | Ineffective communication in ICU impacting treatment timelines, trust, and financial and emotional costs. | Setup of counseling rooms, interactive patient education, and communication training for ICU teams. | Created counseling rooms, modules for patient/family education, and introduced communication training; focused on measurable patient feedback. |
Empathy Listeners (Humanization of ICU Care) | 6 members (nurses, occupational therapist, ICU admin, patient care team) | Dehumanization of ICU environments affecting emotional and psychological well-being of patients, families, and staff. | Training on humanization protocols, empowerment of stakeholders, and open communication policies. | Implemented competency evaluations, family engagement strategies, and humanization-focused communication; used patient feedback tools to refine. |
Table 3. Lahore, Pakistan: Summary of three teams’ composition, problem focus, and proposed solutions.
Empatheon: Transforming ICU Care
A standout result from Lahore was the evolution of the Empathy Listeners initiative into Empatheon, a program dedicated to redefining ICU care through a human-centered and iterative approach (see Table 4). Leveraging PDSA (Plan-Do-Study-Act) cycles, Empatheon systematically tests and refines interventions to address key challenges and ensure sustainable improvements.
Area of Focus | Key Actions/Initiatives | Outcomes/Updates | Next Steps |
|---|---|---|---|
Psychological Support | -Initiated psychology consults with four sessions conducted. | - Addressing burnout and mental health gaps. | - Expand access to psychological support services. - Incorporate structured mental health training for staff. |
Focused Group Sessions | - Held three sessions with ICU SMOs, nursing, housekeeping, and pharmacy staff. | - Key systemic issues resolved. - Greater staff engagement and collaboration. | - Continue focused group sessions to identify new challenges. - Establish routine follow-ups on implemented solutions. |
Mid-Intervention Analysis | - Assessed communication and employee well-being challenges: - Data-driven insights guiding targeted actions for improvement. | - Use insights to prioritize staff training and system-level interventions. - Leverage trends for sustained progress. | |
Communication Training | - Introduced training to improve interactions across teams and with patients and families. | - Enhanced collaboration and patient-family engagement. | - Conduct periodic training refreshers. - Develop scenario-based workshops to strengthen practical skills. |
Feedback Mechanisms | - Established tools to track progress and monitor outcomes. | - Focus on reducing complaints and improving satisfaction scores. | - Use PDSA cycles to refine feedback tools. - Request a dedicated budget for scaling the initiative. |
Table 4. Summary of Empatheon’s recent progress and next steps.
Empatheon’s impact on the double bottom line
Empatheon is redefining ICU care by addressing systemic challenges such as communication gaps, staff well-being, and patient-family dynamics. The program emphasizes the double bottom line, creating both social value through improved care quality, staff morale, and patient-family engagement, and financial impact by reducing inefficiencies, minimizing staff turnover, and fostering operational excellence. Through its iterative approach and focus on continuous improvement, Empatheon serves as a model for human-centered, scalable critical care innovation in resource-constrained environments [7]Thiel, P. (2014). From Zero to One: Notes on Startups, or How to Build the Future. Crown Currency..
Discussion
The workshops demonstrated the transformative potential of Human-Centered Design Thinking (HCDT) in addressing systemic challenges in healthcare delivery, particularly in resource-constrained settings. By leveraging empathy-driven insights and practical, low-cost solutions, participants co-created innovative approaches to complex problems in emergency medicine and intensive care.
Key Insights
- Empathy as the Foundation: Empathy mapping uncovered critical systemic challenges, fostering a deeper understanding of the needs of patients, families, and healthcare teams.
- Collaborative Problem-Solving: The inclusion of diverse, multidisciplinary participants bridged clinical and administrative workflows, enriching the problem-solving process.
- Scalable Innovation: Solutions such as referral coordinators, communication protocols, and empathy-driven ICU improvements laid the groundwork for broader implementation and system-wide transformation.
By emphasizing empathy, collaboration, and resourcefulness, the workshops showcased how practical, adaptive innovation—rooted in Jugaar (fast, frugal, improvised) innovation principles—can be tailored to the unique realities of low- and middle-income countries (LMICs) [4]Salim, Y. (2024). Healthcare Innovation Powered by AI. The Express Tribune..
Low- and middle-income countries (LMICs) face unique systemic challenges in healthcare, education, and public service delivery due to resource constraints, fragmented infrastructures, and socio-cultural complexities. Traditional problem-solving methodologies [8]Innovation & Entrepreneurship. (2023). Comparing human-centered design thinking with traditional problem-solving approaches., while effective in structured settings, often fail to account for the contextual realities and human factors prevalent in these environments. Human-Centered Design Thinking (HCDT) emerges as a more effective and scalable approach in LMICs due to its empathy-driven, participatory, and iterative framework, which contrasts sharply with conventional methodologies such as linear problem-solving models and standard Design Thinking approaches.
HCDT vs. Traditional Problem-Solving Approaches in LMICs
Traditional problem-solving methodologies [8]Innovation & Entrepreneurship. (2023). Comparing human-centered design thinking with traditional problem-solving approaches., such as Six Sigma, Lean, and Root Cause Analysis, emphasize efficiency, standardization, and data-driven decision-making. While these methods are beneficial in high-resource environments, they are often rigid, top-down, and difficult to adapt in LMICs, where problems are frequently dynamic and multifaceted.
HCDT, in contrast, prioritizes [9]IDEO. (2024). What’s the difference between human-centered design and design thinking? IDEO., [10]Mural. (2024). Design thinking vs. human-centered design: A comparative analysis. Mural. community engagement, iterative testing, and local adaptability, making it inherently more resilient and responsive in low-resource settings. For example, in healthcare facilities in LMICs, where limited infrastructure and workforce shortages create bottlenecks, HCDT enables stakeholders—including frontline workers, patients, and administrators—to co-create context-specific, feasible solutions. Unlike traditional models that assume a one-size-fits-all intervention, HCDT allows for real-time feedback and iterative adjustments, ensuring that solutions are both effective and culturally aligned.
HCDT vs. Conventional Design Thinking in LMICs
HCDT extends beyond [9]IDEO. (2024). What’s the difference between human-centered design and design thinking? IDEO., [10]Mural. (2024). Design thinking vs. human-centered design: A comparative analysis. Mural. the model of traditional Design Thinking, by embedding community-based participatory design, resource-conscious prototyping, and locally-driven implementation. For example, in public health interventions in LMICs, traditional Design Thinking may generate technologically advanced but impractical solutions, while HCDT ensures that interventions are low-cost, scalable, and aligned with local ecosystems. This distinction is particularly important in settings where solutions must be socially accepted, economically feasible, and administratively sustainable.
Scalability and Sustainability of HCDT in LMICs
HCDT’s iterative, user-driven approach fosters higher solution adoption and long-term sustainability, making it superior to conventional problem-solving frameworks in LMICs [11]Villanova University. (2025). The power of human-centered design thinking in innovation., [12]Innovation & Entrepreneurship. Comparing human-centered design thinking with traditional problem-solving approaches. Innov Entrep. 2023;12:Article 291.. Key advantages include:
1. Empathy-Driven Problem Identification – Traditional methods often rely on predefined problem statements, which may not capture on-the-ground realities in LMICs. HCDT allows stakeholders to co-define challenges, ensuring relevance and accuracy.
2. Low-Cost, Resource-Conscious Prototyping – Unlike methodologies that require significant infrastructure investment, HCDT emphasizes rapid, low-fidelity prototyping, making it ideal for resource-limited settings.
3. Community Engagement and Co-Creation – In LMICs, top-down solutions often fail due to lack of stakeholder buy-in. HCDT fosters collaborative innovation, ensuring that solutions are culturally and socially integrated.
4. Iterative, Contextual Adaptation – Standard problem-solving models assume stability, whereas LMICs often face dynamic and unpredictable environments. HCDT allows for continuous iteration and refinement, ensuring long-term effectiveness.
When applied to healthcare, education, and social innovation in LMICs, HCDT outperforms both traditional problem-solving methods and conventional Design Thinking by ensuring adaptability, scalability, and user-driven sustainability. Its ability to align interventions with local needs, involve diverse stakeholders, and iterate solutions within real-world constraints makes it an indispensable tool for tackling complex challenges in resource-limited environments.
Conclusion and Next Steps
The success of these workshops highlights the potential of HCDT to foster a culture of empathetic and innovative healthcare delivery. By addressing critical pain points with resourceful and scalable solutions, HCDT provides a replicable framework for sustainable transformation in healthcare systems.
Strategic Outcomes
- Enhanced Quality of Care: Strengthened patient and employee experiences through empathy-driven design.
- Innovation and Diversification: Solutions developed during the workshops demonstrate the potential for broader application and adaptation across varying healthcare settings.
- Scalability and Adaptability: The methodologies emphasize feasibility in resource-constrained environments while remaining adaptable to diverse healthcare contexts.
- Skill Development and Sustainability: Training initiatives and iterative processes create a foundation for continuous improvement and measurable impact.
Future Directions
- Prototype validation: Testing solutions in real-world settings with a focus on measurable outcomes such as patient satisfaction and operational efficiency.
- Scaling training programs: Expanding HCDT workshops to other regions, tailoring modules to address unique challenges and opportunities.
- Integrating HCDT into broader frameworks: HCDT’s methodology aligns with broader innovation management frameworks, such as those exemplified by Innovly, which emphasize scalable, context-driven solutions for sustainable transformation in healthcare.
HCDT’s structured approach not only fosters empathetic and innovative solutions but also addresses inefficiencies that directly impact hospital operations. By optimizing workflows, reducing communication gaps, and improving staff engagement, HCDT has the potential to enhance operational efficiency, indirectly supporting financial sustainability in healthcare systems.
By embedding human-centered design principles into healthcare systems, organizations can create solutions that are empathetic, sustainable, and impactful—setting new benchmarks for innovation and resilience in addressing complex challenges.
Disclosure:
The authors declare no financial or personal conflicts of interest related to this study. The HCDT workshops were conducted at Evercare hospitals in Lekki, Lagos, Nigeria, and Lahore, Pakistan, with institutional support. While Evercare Hospital facilitated the workshops, they had no influence on study design, data collection, analysis, or interpretation. All institutional affiliations are transparently disclosed. No author has received financial compensation, grants, or equity interests that could affect the objectivity of this work.
References
- Mian, A. I. (2021). #C2i-Create-2-Innovate: Expansion From The Merely Technical To The Metaphorical. In A. I. Mian (Ed.), MEDJACK: The Extraordinary Journey of an Ordinary Hack (Kindle Edition). SEED Pvt Ltd.
- Dam, R. F. (2023). The 5 Stages in the Design Thinking Process. Interaction Design Foundation. Retrieved from https://www.interaction-design.org
- Saeed, N., Sulaiman, M., & Mian, A. I. (2023). Human-Centered Design Thinking in the Emergency Department: Channeling the Chaos Together. ACEP Newsroom.
- Salim, Y. (2024). Healthcare Innovation Powered by AI. The Express Tribune.
- World Health Organization. (2022). Trauma Care Manual. Geneva: World Health Organization.
- Kelley, T. (2016). The Art of Innovation: Lessons in Creativity from IDEO. Profile Books.
- Thiel, P. (2014). From Zero to One: Notes on Startups, or How to Build the Future. Crown Currency.
- Innovation & Entrepreneurship. (2023). Comparing human-centered design thinking with traditional problem-solving approaches. Springer Open. Retrieved from https://innovation-entrepreneurship.springeropen.com/articles/10.1186/s13731-023-00291-2.
- IDEO. (2024). What’s the difference between human-centered design and design thinking? IDEO. Retrieved from https://designthinking.ideo.com/faq/whats-the-difference-between-human-centered-design-and-design-thinking
- Mural. (2024). Design thinking vs. human-centered design: A comparative analysis. Mural. Retrieved from https://www.mural.co/blog/design-thinking-vs-human-centered-design
- Villanova University. (2025). The power of human-centered design thinking in innovation. Villanova University. Retrieved from https://www1.villanova.edu/university/professional-studies/about/news-events/2025/0113.html
- Innovation & Entrepreneurship. Comparing human-centered design thinking with traditional problem-solving approaches. Innov Entrep. 2023;12:Article 291. Available from: https://innovation-entrepreneurship.springeropen.com/articles/10.1186/s13731-023-00291-2
Declarations
Ethics approval and consent to participate
Not reported in the submitted manuscript. Editorial confirmation is needed before final PMC packaging.
Consent for publication
Not reported in the submitted manuscript. Editorial confirmation is needed before final PMC packaging.
Availability of data and materials
The workshop evaluation data are not publicly available. De-identified summary materials may be available from the corresponding author on reasonable request, subject to institutional approval.
Funding
No funding was disclosed in onboarding data or article text.
Authors' contributions
Mahreen Sulaiman: Writing - original draft; Writing - review and editing; Conceptualization; Data curation; Methodology | Hira Amran Chowdhry: Writing - review and editing; Data curation | Kazim Ali Tarar: Writing - review and editing; Project administration | Saadia Pervaiz: Writing - review and editing; Methodology | Danish Lalani: Writing - review and editing; Project administration | Ayoola Shonibare: Writing - review and editing | Irfan Khan: Writing - review and editing; Project administration; Supervision | Asad Mian: Writing - original draft; Writing - review and editing; Conceptualization; Methodology; Project administration; Data curation; Investigation
Competing interests
No conflict of interest was disclosed in onboarding data or article text.