


ABSTRACT
Background: Innovation is a key driver of healthcare transformation, particularly in low-resource settings where systemic constraints often hinder service delivery. Assessing innovation capacities among healthcare employees can inform workforce development strategies. This study applies the previously validated Innovation Skills Assessment (ISA) tool to examine workforce innovation potential at a tertiary care hospital in Pakistan, offering insights for targeted capacity-building interventions.
Methods: A cross-sectional survey was conducted at Mukhtar A. Sheikh Hospital in Multan, Pakistan, using the ISA tool adapted from the General Innovation Skills Aptitude Test. The survey captured demographic data and assessed innovation skills across four pillars: idea generation, risk-taking, interpersonal relationships, and idea implementation. A total of 250 electronic surveys were distributed via hospital communication channels, with 161 responses (64% response rate). Responses were rated on a 5-point Likert scale, and mean scores with standard deviations were calculated for each pillar. Descriptive statistics were used to explore observable trends across age, gender, education level, and job designation, without formal hypothesis testing.
Results: Participants aged 36–45 years had the highest overall mean scores (4.48 ± 0.31), with notable strengths in idea generation (4.48 ± 0.31) and implementation (4.53 ± 0.33). Males showed higher average scores across all pillars, with interpersonal relationships as the strongest domain (4.49 ± 0.42). Participants with intermediate education reported higher mean scores in creativity and risk-taking (4.36 ± 0.45 and 4.20 ± 0.57, respectively). These patterns suggest potential demographic influences on innovation capacities.
Conclusion: The ISA tool can be feasibly applied to map innovation skills within healthcare workforces in low-resource contexts. The identified trends may help guide workforce development through tailored training and institutional policies that promote a culture of innovation.
Keywords: Innovation Skills Assessment, Healthcare Workforce, Low-Resource Settings, Human-Centered Design, Capacity-Building, Pakistan, Benchmarking, Workforce Innovation
BACKGROUND
Innovation is a critical driver of healthcare transformation, particularly in low- and middle-income countries (LMICs) where systemic challenges such as resource scarcity, fragmented infrastructure, and workforce shortages limit access to high-quality care [1]Maghsoudi S, Duffield C, Wilson DJ. Innovation evaluation: past and current models and a framework for infrastructure projects. Int J Innov Sci. 2015;7(4):281-97.–[2]Baker S, Mehmood A. Social innovation and the governance of sustainable places. Local Environ. 2015;20(3):321-34.. In such contexts, introducing innovative approaches is not merely advantageous but often essential for sustaining and improving service delivery, patient outcomes, and system resilience [3]Bhattacharyya O, Khor S, McGahan A, Dunne D, Daar AS, Singer PA, et al. Innovative health service delivery models in low and middle income countries—what can we learn from the private sector? Health Res Policy Syst. 2010;8:1-11.. Structured innovation frameworks, grounded in evidence and adapted to local realities, can optimize processes, streamline care pathways, and embed continuous improvement within healthcare systems [4]Kabene SM, Orchard C, Howard JM, Soriano MA, Leduc R. The importance of human resources management in health care: a global context. Hum Resour Health. 2006;4:1-17..
Traditional top-down models of healthcare innovation frequently overlook the tacit knowledge and context-specific insights of frontline workers [5]Tahir HN, Allana ZA, MacKay D, Farooqi W, Mian AI. Innovation Skills Assessment and Variation among Healthcare Employees in the Emergency Department: A Cross-sectional Study. Eurasian J Emerg Med. 2024;23(1):26-34.. In contrast, grassroots and participatory approaches, where employees at all levels contribute to problem-solving, can yield solutions that are both locally relevant and scalable [6]Greenhalgh T, Wherton J, Papoutsi C, Lynch J, Hughes G, A'Court C, et al. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res. 2017;19(11):e367.–[8]Crossan MM, Apaydin M. A multi‐dimensional framework of organizational innovation: a systematic review of the literature. J Manage Stud. 2010;47(6):1154-91.. These approaches foster ownership, adaptability, and long-term sustainability, which are particularly vital in resource-constrained environments.
Despite the recognized value of innovation in healthcare, there remains a significant gap in assessing and benchmarking innovation capacities among healthcare workers in LMICs [3]Bhattacharyya O, Khor S, McGahan A, Dunne D, Daar AS, Singer PA, et al. Innovative health service delivery models in low and middle income countries—what can we learn from the private sector? Health Res Policy Syst. 2010;8:1-11.,[7]Edwards N, Kaseje D, Kahwa E, Klopper H, Mill J, Webber J, et al. Strengthening health systems in low- and middle-income countries: a framework for action. Glob Public Health. 2015;10(4):489-500.. Understanding how workforce characteristics, such as age, gender, education, and job designation, affect innovation potential is critical for designing targeted interventions [7]Edwards N, Kaseje D, Kahwa E, Klopper H, Mill J, Webber J, et al. Strengthening health systems in low- and middle-income countries: a framework for action. Glob Public Health. 2015;10(4):489-500.,[8]Crossan MM, Apaydin M. A multi‐dimensional framework of organizational innovation: a systematic review of the literature. J Manage Stud. 2010;47(6):1154-91.. Without structured assessment mechanisms, healthcare organizations risk missing opportunities to identify, nurture, and strategically deploy innovation skills [5]Tahir HN, Allana ZA, MacKay D, Farooqi W, Mian AI. Innovation Skills Assessment and Variation among Healthcare Employees in the Emergency Department: A Cross-sectional Study. Eurasian J Emerg Med. 2024;23(1):26-34.,[8]Crossan MM, Apaydin M. A multi‐dimensional framework of organizational innovation: a systematic review of the literature. J Manage Stud. 2010;47(6):1154-91..
The Innovation Skills Assessment (ISA) tool, adapted from the General Innovation Skills Aptitude Test [9]Centre for Business Innovation. (2013). General Innovation Skills Aptitude Test 2.0. The Conference Board of Canada., offers a structured means of measuring workforce innovation competencies. It has been applied in LMIC healthcare contexts, including emergency department settings, to map skills across four core domains: idea generation, risk-taking, interpersonal relationships, and idea implementation [5]Tahir HN, Allana ZA, MacKay D, Farooqi W, Mian AI. Innovation Skills Assessment and Variation among Healthcare Employees in the Emergency Department: A Cross-sectional Study. Eurasian J Emerg Med. 2024;23(1):26-34.. However, its application at a whole-hospital level remains underexplored, particularly in Pakistan, where empirical data on healthcare innovation competencies are scarce.
This study addresses this gap by employing the ISA tool to assess hospital-wide workforce innovation capacities in a tertiary care facility in Multan, Pakistan. The aim is exploratory rather than hypothesis-driven, focusing on descriptive trends instead of inferential statistical comparisons. By mapping innovation potential across demographic groups, the study generates baseline insights to inform tailored capacity-building initiatives and organizational policies aimed at strengthening innovation culture in low-resource healthcare environments.
METHODS
Study Design and Setting
This cross-sectional, descriptive study was conducted at Mukhtar A. Sheikh Hospital (MASH) in Multan, Pakistan [10]Mukhtar A. Sheikh Hospital. About Us. Mukhtar A. Sheikh Hospital Website., a multidisciplinary tertiary care facility. MASH was selected as the research site due to its structured institutional focus on innovation, ongoing workforce development programs, and its diverse mix of clinical and non-clinical professionals. As a relatively newer hospital in the region, MASH has prioritized progressive healthcare models, making it a suitable setting to assess workforce innovation capacities in an LMIC context. The study aimed to identify broad trends in innovation skills across various professional groups rather than test predefined hypotheses, generating insights that could inform targeted capacity-building initiatives.
Participants and Sampling
The study included both clinical and non-clinical staff to ensure a hospital-wide assessment of innovation skills. Clinical participants comprised doctors, nurses, and technicians, while non-clinical participants included administrators, operations personnel, and support staff. Employees with at least six months of tenure at MASH were included to ensure familiarity with institutional workflows and work culture. Individuals with prior formal training in innovation or entrepreneurship were excluded to minimize bias in self-reported innovation competencies.
A non-probability convenience sampling approach was used. Electronic surveys were distributed through the hospital’s official email lists and WhatsApp communication groups to maximize accessibility. To encourage participation, two weekly reminders were sent following the initial distribution. Out of 250 surveys distributed, 161 completed responses were received, yielding a response rate of 64%, which is considered robust for survey-based research of this nature.
Innovation Skills Assessment Tool
The Innovation Skills Assessment (ISA) tool was used to evaluate workforce innovation capacities across four key pillars: idea generation, risk-taking, interpersonal relationships, and idea implementation. Developed through Innovly [11]Innovly. Driving Innovation in Healthcare and Organizations. Innovly Website., a startup focused on innovation management in healthcare and other organizational settings, ISA was adapted from the General Innovation Skills Aptitude Test (GISAT 2.0), a validated framework for assessing innovation competencies across various professional sectors [9]Centre for Business Innovation. (2013). General Innovation Skills Aptitude Test 2.0. The Conference Board of Canada.. The ISA tool was modified further to reflect healthcare-specific challenges, including hospital workflows, decision-making constraints, and team-based collaboration [5]Tahir HN, Allana ZA, MacKay D, Farooqi W, Mian AI. Innovation Skills Assessment and Variation among Healthcare Employees in the Emergency Department: A Cross-sectional Study. Eurasian J Emerg Med. 2024;23(1):26-34..
To ensure its relevance in a hospital setting, modifications were made based on expert consultations and pilot testing at the Aga Khan University Hospital in Karachi, Pakistan. These adjustments refined survey phrasing, contextualized innovation-related questions for clinical and non-clinical staff, and ensured applicability across various healthcare roles. The final version of the tool maintained core innovation competency pillars while improving its specificity for the healthcare workforce.
The ISA survey consisted of three sections: demographic data, professional role and employment characteristics, and an innovation skills assessment. Demographic information included participant age, gender, education level, job designation, and years of experience. The professional role and employment characteristics section distinguished between clinical and non-clinical staff. The innovation skills assessment component utilized a five-point Likert scale, with responses ranging from one (strongly disagree) to five (strongly agree), allowing for a standardized evaluation of participants' self-perceived innovation capabilities.
Survey Administration and Data Collection
The survey was administered electronically, ensuring ease of access for all participants. Confidentiality was maintained by anonymizing all responses, with no identifying information collected. Participants were provided with a brief study overview, including its objectives and the voluntary nature of participation, before accessing the survey.
Statistical Analysis
Given the descriptive and exploratory nature of the study, statistical analysis focused on summarizing workforce innovation trends rather than performing inferential hypothesis testing. Likert-scale responses were analyzed using means and standard deviations to capture variations in self-reported innovation capacities. Data were stratified based on demographic variables, including age, gender, education level, and job designation, to assess differences in innovation skill profiles across workforce subgroups. Results were visually represented using bar charts to highlight emerging patterns and actionable insights.
While inferential statistical testing can offer additional depth, this study was not designed to establish statistically significant differences. Instead, the analysis was structured to identify broad workforce trends that could inform future interventions aimed at fostering a culture of innovation within healthcare organizations.
Ethical Considerations
The study did not involve direct patient contact or any intervention that posed a risk to participants. Given the nature of the survey and the low-risk profile of the study, approval was obtained from the Senior Administration team at MASH in lieu of an institutional review board, which the hospital does not have. Informed consent was obtained from all participants before survey completion. To maintain confidentiality and ethical integrity, no personal identifiers were collected, and responses were anonymized before analysis.
RESULTS
A total of 161 employees participated in the study, representing a balanced mix of clinical (52.8%) and non-clinical (47.2%) staff. Of the total participants, 60% were male and 40% were female, reflecting a gender distribution common in many healthcare settings. The largest age group was 25–35 years (59%), followed by 36–45 years (13%), with only 2.6% of participants aged 46 years or older. The youngest group, those under 25 years, accounted for 25.4% of the workforce. The detailed sociodemographic characteristics of the study participants are presented in Table 1.
Table 1: Sociodemographic characteristics of study participants
Demographic parameters | n | % |
|---|---|---|
Age | ||
<25 years | 41 | 25.4 |
25–35 years | 95 | 59.0 |
36–45 years | 21 | 13.0 |
46–55 years | 3 | 2.0 |
>55 years | 1 | 0.6 |
Total (N) | 161 | 100 |
Gender | ||
Female | 64 | 40.0 |
Male | 97 | 60.0 |
Total (N) | 161 | 100 |
Education Level | ||
Secondary school | 2 | 1.2 |
Matric | 8 | 5.0 |
Intermediate | 18 | 11.2 |
Undergraduate | 43 | 26.7 |
Postgraduate | 84 | 52.2 |
Doctorate | 6 | 3.7 |
Total (N) | 161 | 100 |
Currently studying | ||
No | 123 | 76.4 |
Yes | 38 | 23.6 |
Total (N) | 161 | 100 |
Length of employment | ||
Less than 1 year | 48 | 29.8 |
1–2 years | 56 | 34.8 |
2–3 years | 43 | 26.7 |
3 years or more | 14 | 8.7 |
Total (N) | 161 | 100 |
Placement | ||
Non-clinical | 76 | 47.2 |
Clinical | 85 | 52.8 |
Total (N) | 161 | 100 |
In terms of educational background, 52.2% of participants held postgraduate degrees, while 26.7% had undergraduate qualifications. A smaller proportion (11.2%) had completed intermediate-level education, while only 1.2% had secondary school education. A notable proportion (23.6%) were currently pursuing further studies. Workforce tenure at MASH was relatively short, with 64.6% of participants having less than two years of service at the hospital. Only 8.7% had three or more years of experience, indicating a young and relatively new workforce.
Innovation Skills Assessment Scores
ISA scores were analyzed across the four core pillars of innovation:
- Pillar I: Generating ideas
- Pillar II: Taking calculated risks and being entrepreneurial
- Pillar III: Developing and maintaining interpersonal relationships
- Pillar IV: Turning ideas into products, processes, and services
As shown in Table 2, participants aged 36–45 demonstrated the highest innovation scores across all pillars, excelling particularly in idea generation (Pillar I) and idea implementation (Pillar IV). Males scored slightly higher than females in all pillars. Postgraduates achieved the highest overall scores, especially in interpersonal relationships (Pillar III), while those with intermediate-level education showed notable strengths in idea generation and risk-taking. Participants with three or more years of experience recorded the strongest scores across all pillars.
Table 2: Stratified Innovation Skills Assessment (ISA) scores by demographic characteristics
Variable | Pillar I | Pillar II | Pillar III | Pillar IV |
|---|---|---|---|---|
Age (years) | ||||
<25 years | 4.27 ± 0.44 | 4.01 ± 0.52 | 4.41 ± 0.52 | 4.35 ± 0.50 |
25–35 years | 4.38 ± 0.44 | 4.11 ± 0.48 | 4.44 ± 0.46 | 4.40 ± 0.47 |
36–45 years | 4.48 ± 0.31 | 4.32 ± 0.43 | 4.63 ± 0.31 | 4.53 ± 0.33 |
>46 years | 4.44 ± 0.35 | 4.14 ± 0.50 | 4.42 ± 0.45 | 4.28 ± 0.40 |
Gender | ||||
Female | 4.34 ± 0.42 | 4.04 ± 0.47 | 4.39 ± 0.52 | 4.36 ± 0.49 |
Male | 4.38 ± 0.43 | 4.16 ± 0.50 | 4.49 ± 0.42 | 4.43 ± 0.44 |
Education Level | ||||
Secondary school/Matric | 4.02 ± 0.50 | 3.94 ± 0.61 | 4.21 ± 0.46 | 4.25 ± 0.40 |
Intermediate | 4.36 ± 0.45 | 4.20 ± 0.57 | 4.43 ± 0.61 | 4.40 ± 0.62 |
Undergraduate | 4.35 ± 0.41 | 4.08 ± 0.46 | 4.45 ± 0.46 | 4.38 ± 0.47 |
Postgraduate | 4.42 ± 0.42 | 4.12 ± 0.49 | 4.51 ± 0.43 | 4.45 ± 0.43 |
Doctorate | 4.28 ± 0.14 | 4.07 ± 0.22 | 4.23 ± 0.43 | 4.23 ± 0.39 |
Currently studying | ||||
No | 4.37 ± 0.41 | 4.11 ± 0.46 | 4.47 ± 0.43 | 4.42 ± 0.43 |
Yes | 4.35 ± 0.46 | 4.11 ± 0.58 | 4.42 ± 0.57 | 4.34 ± 0.56 |
Experience | ||||
<1 year | 4.42 ± 0.40 | 4.08 ± 0.47 | 4.52 ± 0.41 | 4.52 ± 0.44 |
1–2 years | 4.33 ± 0.45 | 4.08 ± 0.51 | 4.42 ± 0.50 | 4.30 ± 0.48 |
2–3 years | 4.34 ± 0.45 | 4.14 ± 0.49 | 4.41 ± 0.49 | 4.39 ± 0.48 |
≥3 years | 4.40 ± 0.31 | 4.25 ± 0.48 | 4.51 ± 0.44 | 4.45 ± 0.35 |
Job designation | ||||
Doctor | 4.51 ± 0.43 | 4.23 ± 0.51 | 4.58 ± 0.37 | 4.60 ± 0.36 |
Nursing staff | 4.32 ± 0.40 | 4.09 ± 0.49 | 4.41 ± 0.48 | 4.39 ± 0.49 |
Others | 4.37 ± 0.43 | 4.10 ± 0.49 | 4.46 ± 0.47 | 4.38 ± 0.46 |
Across the entire workforce, interpersonal relationship skills (Pillar III) were the highest-rated innovation competency across all demographic groups. Participants with intermediate-level education performed well in idea generation and risk-taking despite lower formal qualifications. Those with less than one year of experience had the highest scores in risk-taking, while employees with three or more years of tenure consistently recorded the strongest scores across all pillars. Doctors scored highest overall, particularly in idea generation and interpersonal relationships, followed by nursing staff in team-related skills.
Figures 1–4 illustrate the distribution of ISA scores across gender, age groups, education levels, and length of service, highlighting differences in performance for each of the four pillars of innovation.
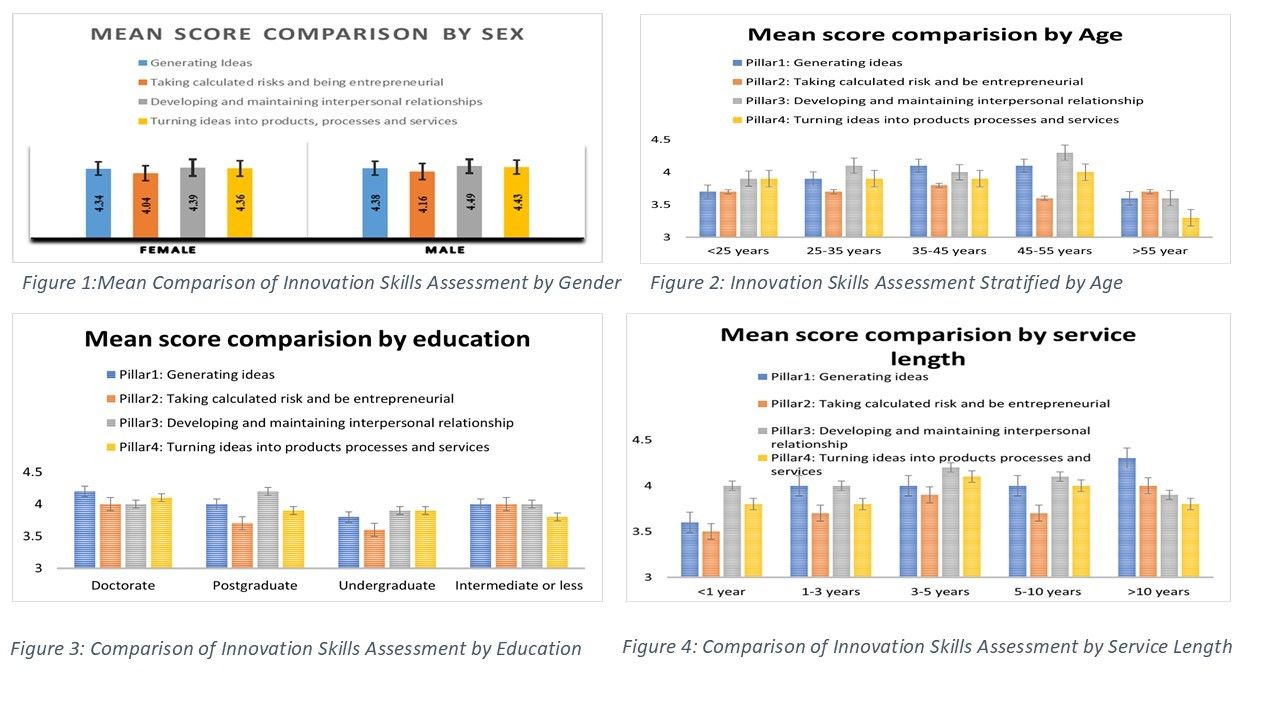
Figures 1–4. Stratified ISA scores across key demographic variables, including gender (Figure 1), age groups (Figure 2), education levels (Figure 3), and length of service/tenure (Figure 4). Each figure illustrates the distribution of innovation competencies across the four ISA pillars: idea generation, risk-taking, interpersonal relationships, and idea implementation—highlighting how different workforce segments perform in innovation-related skills. These trends help identify potential gaps and strengths in innovation capacities across the hospital workforce.
DISCUSSION
This descriptive, exploratory study highlights that healthcare systems in low- and middle-income countries (LMICs) encounter persistent obstacles to innovation, primarily stemming from financial limitations, inadequate infrastructure, and workforce issues. These barriers hinder the generation, implementation, and sustainability of creative solutions that can improve patient care and operational efficiency. Data-driven assessments such as the Innovation Skills Assessment (ISA) help identify workforce skill gaps and inform targeted actions [5]Tahir HN, Allana ZA, MacKay D, Farooqi W, Mian AI. Innovation Skills Assessment and Variation among Healthcare Employees in the Emergency Department: A Cross-sectional Study. Eurasian J Emerg Med. 2024;23(1):26-34.. Applying such tools enables hospitals to track innovation trends over time and adopt strategies that support creativity and problem-solving across healthcare teams. While the ISA tool has been validated in emergency department settings, this study applied it hospital-wide, demonstrating its potential as a structured method to assess innovation strengths and gaps across diverse roles.
Learning from LMIC-based innovation skill evaluations can have global relevance. Low-tech, high-impact interventions first developed in LMICs have been adapted successfully in high-income settings, particularly in cost-effective patient care models and digital health innovations [3]Bhattacharyya O, Khor S, McGahan A, Dunne D, Daar AS, Singer PA, et al. Innovative health service delivery models in low and middle income countries—what can we learn from the private sector? Health Res Policy Syst. 2010;8:1-11.. Building local innovation ecosystems in LMIC hospitals may enhance service delivery and contribute to global healthcare improvement [12]Ishimwe MCS, Kiplagat J, Knowlton AK, Livinski AA, Kupfer LE. Reversing the trend: a scoping review of health innovation transfer or exchange from low-and middle-income countries to high-income countries. BMJ Global Health. 2023;8(Suppl 7):e013583..
One pattern observed was variation in innovation competencies across demographic groups, suggesting areas for targeted workforce development. Younger employees, especially those under 25 years of age, tended to have lower innovation scores, potentially reflecting limited professional experience and reduced decision-making authority. These findings align with the need for structured mentorship and experiential learning to develop creative capacities early in a career. Our preliminary work on innovation capacity building in university-based academia supports this approach (unpublished data).
Mid-career professionals (36–45 years) showed the strongest innovation scores, consistent with the idea that professional maturity, leadership responsibilities, and accumulated experience can enhance problem-solving and risk-taking abilities. Research on ‘silver age innovators’ notes that older employees may leverage long-term contextual knowledge to refine and improve healthcare systems [13]Östlund B. Silver age innovators: a new approach to old users. The Silver Market Phenomenon: Marketing and Innovation in the Aging Society. 2011:15-26.. Contrary to assumptions that younger employees are inherently more innovative, prior studies indicate that, with the right opportunities, senior professionals actively contribute to early-stage service design and problem-solving [13]Östlund B. Silver age innovators: a new approach to old users. The Silver Market Phenomenon: Marketing and Innovation in the Aging Society. 2011:15-26.,[14]Essén A, Östlund B. Laggards as innovators? Old users as designers of new services & service systems. Int J Design. 2011;5(3).. These findings point to the importance of sustaining innovation training opportunities throughout a professional’s career.
Gender-based differences in innovation scores were also noted, with male employees scoring higher across all four ISA pillars compared to female employees. This aligns with organizational research suggesting that men often hold leadership roles more frequently, giving them greater exposure to decision-making and strategic innovation [4]Kabene SM, Orchard C, Howard JM, Soriano MA, Leduc R. The importance of human resources management in health care: a global context. Hum Resour Health. 2006;4:1-17.. However, this disparity likely reflects structural and cultural barriers rather than inherent differences in innovation potential. Women, despite forming the majority of the global healthcare workforce, remain underrepresented in leadership positions, often due to institutional constraints rather than capability gaps [14]Essén A, Östlund B. Laggards as innovators? Old users as designers of new services & service systems. Int J Design. 2011;5(3).. Addressing such barriers through inclusive leadership pathways and equitable opportunities is key to closing this gap.
Education and professional experience also appeared to influence innovation competencies. Participants with intermediate-level education scored higher in creativity and risk-taking, suggesting that hands-on experience can play a stronger role than formal academic training in fostering innovation [15]Fadzil NM, Kamarudin WW. The Influence of Creativity and Willingness to Take Risks on Students’ Entrepreneurial Intention. Int J Acc. 2022;7(43):412-20.. Postgraduate-educated participants excelled in interpersonal relationships, emphasizing the importance of collaboration in driving healthcare innovation [1]Maghsoudi S, Duffield C, Wilson DJ. Innovation evaluation: past and current models and a framework for infrastructure projects. Int J Innov Sci. 2015;7(4):281-97.,[15]Fadzil NM, Kamarudin WW. The Influence of Creativity and Willingness to Take Risks on Students’ Entrepreneurial Intention. Int J Acc. 2022;7(43):412-20.,[16]Graciano P, Lermen FH, Reichert FM, Padula AD. The impact of risk-taking and creativity stimuli in education towards innovation: A systematic review and research agenda. Thinking Skills and Creativity. 2023;47:101220.. Those with more than three years of professional experience performed better in risk-taking and idea implementation [17]Caro-Gonzalez A. Establishing a culture of innovation and risk-taking. Transformative Governance for the Future: Navigating Profound Transitions: Springer; 2023. p. 47-56., reinforcing the value of cumulative experience in supporting innovation [18]Leverage Network Inc Mid-Career Odyssey: Training programs for experienced professionals in leadership and innovation The Leverage Network 2024..
This study provides insight into workforce innovation patterns but has several limitations. The one-week data collection period may not capture variations in innovation skills over time. Factors such as workload changes, institutional dynamics, and seasonal shifts could influence results. Findings are from a single site and may not be generalizable to other healthcare settings, including public or rural institutions. Although the 64% response rate is reasonable, non-response bias was not assessed. Future research should explore differences between respondents and non-respondents to strengthen conclusions. As a self-reported survey, the ISA may be subject to response bias, and participants’ perceived skills may not match objective performance metrics. Future studies incorporating observational data or external evaluations could improve validity. Additionally, formal effect size calculations or comparative statistical analyses were not performed, so findings are best interpreted as descriptive trends rather than definitive inferences.
CONCLUSION
This study demonstrates the utility of the ISA tool in evaluating hospital-wide innovation capacities in an LMIC setting. Findings point to mid-career professionals as strong contributors to innovation and highlight gaps linked to gender, education, and job function. Addressing these disparities through targeted training, mentorship, and inclusive policies can strengthen workforce innovation potential. Broader, multi-site, and longitudinal applications of the ISA could deepen understanding of how innovation competencies evolve over time.
Declarations
Ethics approval and consent to participate
The manuscript reports that approval was obtained from the Senior Administration team at MASH in lieu of an institutional review board, which the hospital does not have. Responses were anonymized before analysis.
Consent for publication
The manuscript reports that informed consent was obtained from all participants before survey completion.
Availability of data and materials
The anonymized survey data are not publicly available. De-identified summary data may be available from the corresponding author on reasonable request, subject to institutional approval.
Competing interests
No conflict of interest was disclosed in onboarding data or article text.
Funding
No funding was disclosed in onboarding data or article text.
Authors' contributions
Ahmed Raheem: Writing - original draft; Writing - review and editing; Conceptualization; Data curation; Formal analysis; Validation | Hasan N Tahir: Writing - review and editing; Conceptualization; Project administration; Methodology | Zeeshan Ahsan Allana: Writing - original draft; Conceptualization; Methodology; Data curation; Investigation; Project administration | Mahreen Sulaiman: Writing - original draft; Supervision; Project administration; Resources; Investigation | Irfan Khan: Writing - original draft; Project administration; Resources; Visualization; Conceptualization | Haseeb Sajid: Writing - review and editing; Investigation; Software; Methodology; Project administration | Mehdia Nadeem Rajab Ali: Writing - original draft; Writing - review and editing; Resources; Conceptualization; Project administration; Investigation | Asad I Mian: Writing - original draft; Writing - review and editing; Conceptualization; Investigation; Methodology; Validation; Project administration; Supervision
REFERENCES
- Maghsoudi S, Duffield C, Wilson DJ. Innovation evaluation: past and current models and a framework for infrastructure projects. Int J Innov Sci. 2015;7(4):281-97.
- Baker S, Mehmood A. Social innovation and the governance of sustainable places. Local Environ. 2015;20(3):321-34.
- Bhattacharyya O, Khor S, McGahan A, Dunne D, Daar AS, Singer PA, et al. Innovative health service delivery models in low and middle income countries—what can we learn from the private sector? Health Res Policy Syst. 2010;8:1-11.
- Kabene SM, Orchard C, Howard JM, Soriano MA, Leduc R. The importance of human resources management in health care: a global context. Hum Resour Health. 2006;4:1-17.
- Tahir HN, Allana ZA, MacKay D, Farooqi W, Mian AI. Innovation Skills Assessment and Variation among Healthcare Employees in the Emergency Department: A Cross-sectional Study. Eurasian J Emerg Med. 2024;23(1):26-34.
- Greenhalgh T, Wherton J, Papoutsi C, Lynch J, Hughes G, A'Court C, et al. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res. 2017;19(11):e367.
- Edwards N, Kaseje D, Kahwa E, Klopper H, Mill J, Webber J, et al. Strengthening health systems in low- and middle-income countries: a framework for action. Glob Public Health. 2015;10(4):489-500.
- Crossan MM, Apaydin M. A multi‐dimensional framework of organizational innovation: a systematic review of the literature. J Manage Stud. 2010;47(6):1154-91.
- Centre for Business Innovation. (2013). General Innovation Skills Aptitude Test 2.0. The Conference Board of Canada. https://www.accaglobal.com/content/dam/ACCA_Global/professional-insights/integrative-thinking/General%20Innovation%20Aptitude%20Test.pdf
- Mukhtar A. Sheikh Hospital. About Us. Mukhtar A. Sheikh Hospital Website. Accessed March 12, 2025. Available from: https://mashospital.org/.
- Innovly. Driving Innovation in Healthcare and Organizations. Innovly Website. Accessed March 12, 2025. Available from: https://innovly.net/.
- Ishimwe MCS, Kiplagat J, Knowlton AK, Livinski AA, Kupfer LE. Reversing the trend: a scoping review of health innovation transfer or exchange from low-and middle-income countries to high-income countries. BMJ Global Health. 2023;8(Suppl 7):e013583.
- Östlund B. Silver age innovators: a new approach to old users. The Silver Market Phenomenon: Marketing and Innovation in the Aging Society. 2011:15-26.
- Essén A, Östlund B. Laggards as innovators? Old users as designers of new services & service systems. Int J Design. 2011;5(3).
- Fadzil NM, Kamarudin WW. The Influence of Creativity and Willingness to Take Risks on Students’ Entrepreneurial Intention. Int J Acc. 2022;7(43):412-20.
- Graciano P, Lermen FH, Reichert FM, Padula AD. The impact of risk-taking and creativity stimuli in education towards innovation: A systematic review and research agenda. Thinking Skills and Creativity. 2023;47:101220.
- Caro-Gonzalez A. Establishing a culture of innovation and risk-taking. Transformative Governance for the Future: Navigating Profound Transitions: Springer; 2023. p. 47-56.
- Leverage Network Inc Mid-Career Odyssey: Training programs for experienced professionals in leadership and innovation The Leverage Network 2024 Available from: https://theleveragenetworkinccom/mid-career-odyssey.