

INTRODUCTION
The intersection of healthcare access and social services utilization is a critical frontier for combating health disparities within the United States healthcare system. Federal benefit programs, including the Lifeline program, aimed at addressing broadband phone and internet access, constitute fundamental components of the social safety-net, collectively serving millions of Americans.[1]Headrick, G., Ruth, A., White, S. A., Ellison, C., Seligman, H., Bleich, S. N., et al. (2022). Integration and coordination across public benefit programs: Insights from state and local government leaders in the United States. Preventive medicine reports, 31, 102077. https://doi.org/10.1016/j.pmedr.2022.102077 The Lifeline program, created in 1985 by the federal government, provides a subsidy of $9.25 per month to qualifying individuals to support their internet access, filling a gap in digital connectivity.[2]Federal Communications Commission. (2012, January 27). Lifeline Program for Low-Income Consumers. Federal Communications Commission. https://www.fcc.gov/general/lifeline-program-low-income-consumers Economic assistance programs, including Lifeline, often operate via fragmented and convoluted infrastructures. Opaque application processes, coupled with administrative barriers, such as understaffing and excessive clerical burden, create significant obstacles to access.[3]Jones, C. H., & Dolsten, M. (2024). Healthcare on the brink: navigating the challenges of an aging society in the United States. Npj Aging, 10(1), 1–10. https://doi.org/10.1038/s41514-024-00148-2 These challenges are exacerbated within vulnerable populations facing limitations in digital literacy, language proficiency, and program awareness. The result of these constraints is under-enrollment among eligible individuals and families.[4]Lim, H. A., Lee, J. S. W., Lim, M. H., Teo, L. P. Z., Sin, N. S. W., Lim, R. W., et al. (2022). Bridging Connectivity Issues in Digital Access and Literacy: Reflections on Empowering Vulnerable Older Adults in Singapore. JMIR Aging, 5(2), e34764. https://doi.org/10.2196/34764
In response to these systemic challenges, digital enrollment interventions have shown promise in expanding benefit access. Previous models demonstrate the success of digital, text-based interventions in supporting community health. Kaiser Permanente, in partnership with the Center for Health Law and Policy Innovation of Harvard Law School, conducted a digital outreach campaign in California in 2019 to support enrollment in the Supplemental Nutrition Assistance Program (SNAP) and the Special Supplemental Nutrition Program for Women, Infants & Children (WIC). By 2021, their program had helped over 82,000 individuals apply for benefits.[5]Health Law Lab. (2021). Text message outreach to support SNAP and WIC enrollment in California. Retrieved November 19, 2024, from https://www.healthlawlab.org/wp-content/uploads/2021/10/Text-Message-Outreach-to-Support-SNAP-and-WIC-Enrollment-2021.pdf An effort between Benefits Data Trust (BDT) and the Center on Budget and Policy Priorities (CBPP), piloted text outreach in four states – Colorado, Massachusetts, Montana, and Virginia – to connect eligible families to WIC. Out of 35,908 people who received texts in Virginia, over 25% interacted with the messages in some way (any response other than opting out), and 9% of the total recipients successfully enrolled in the program. Similar rates were seen in the other three states. The authors argued that text outreach is cost-effective, and also that it is low-maintenance.[6]Center on Budget and Policy Priorities & Benefits Data Trust. (2022). Maximizing WIC participation with text messaging: A guide for WIC agencies. Digital Government Hub. https://digitalgovernmenthub.org/wp-content/uploads/2022/07/cbpp-bdt-wic-texting-guide.pdf
Furthermore, Code for America, a non-profit organization linking technology to government, built a text-messaging service with Louisiana in 2018 to increase enrollments and renewals in four government assistance programs – Medicaid, SNAP, WIC, and Temporary Assistance for Needy Families. Their results were impressive: 27,000 residents agreed to receive text messages during a nine-month pilot, and since then, over 50 million texts have been sent.[7]Code for America. (2024, December 17). Simplifying Communications to Help People Maintain Benefits in Louisiana — Code for America. Code for America. https://codeforamerica.org/success-stories/simplifying-communications-to-help-people-maintain-benefits-in-louisiana/ These studies demonstrate the ability of digital outreach methods to reach and potentially support the enrollment in economic assistance programs of large numbers of individuals in relatively short time frames.
Link Health, a nonprofit organization operating within the Greater Boston metropolitan area, has implemented an innovative intervention model that reconceptualizes the integration of federal benefits access within healthcare delivery systems.[8]Joseph, N. P., Hider, A. M., Contreras, D., Velasquez, D. E., & Martin, A. (2023). Bridging the digital divide through on-site, health center-based internet clinics. NEJM Catalyst. https://doi.org/10.1056/CAT.23.0099 Through strategic partnerships with federally qualified health centers (FQHCs) across economically disadvantaged neighborhoods in Boston—including East Boston, Roxbury, Dorchester, and Mattapan—Link Health has developed a framework for benefit enrollment that transcends traditional service delivery paradigms. This framework encompasses three distinct but complementary approaches: sophisticated digital outreach via proactive text-messaging campaigns, active in-person enrollment with face-to-face patient navigators at health clinics, and systematic passive enrollment via self-service online forms. In this analysis, we describe the digital outreach mechanism’s success in reaching disadvantaged populations, as well as streamlining and significantly reducing the time needed to enroll into assistance programs.
Through examination of Link Health’s Lifeline enrollment data, demographic reach, and financial impact metrics, we evaluate the effectiveness of embedding benefits access within existing private messaging frameworks. The findings presented contribute to the growing body of literature on digital-based healthcare interventions addressing social determinants of health (SDOH), while providing actionable insights for healthcare administrators and public health practitioners.
METHODS
The research protocol for this study was reviewed by the Northeastern Institutional Review Board (IRB) and determined to fall outside the definition of human subjects research. As a result, this secondary analysis of Link Health operational data required no additional IRB approval prior to the commencement of the research activities.
From June 2024 to December 2024, Link Health conducted a targeted text-messaging campaign aimed at enrolling patients from seven partner community health centers into the Lifeline program. This study employed a digital engagement model to complement and replicate the goals of the existing in-person outreach program administered by Link Health. In total, 68,529 Boston patients received messages from their partner clinics, including Duffy Health Center, Fenway Health Center, SSTAR Health Center, Charles River Community Health Center, Community Health Connections, Upham’s Corner Health Center, and Lowell Community Health Center.
Partner community health clinics served as intermediaries to connect with their patient populations. Patients whose records indicated prior enrollment in programs such as Medicaid, Medicare, and/or SNAP were considered adjunctively eligible, meaning that they would automatically qualify for other benefits programs based on their past program participation. These adjunctively eligible individuals were hence included in this study. These patients received an initial text message from their clinic containing information about Link Health, the Lifeline program, and a link to initiate further communication with the Link Health team. When patients clicked the link, a new text conversation opened within their messaging application, displaying a pre-prepared message stating: “Send this text to Link Health to enroll in the Lifeline program,” with translations in Spanish and Portuguese. By clicking the icon signifying "send," the patient’s message was routed to the Link Health digital team via DaisyChain, a web-based communication platform that allows Link Health’s digital team to simulate text conversations from their computer or other device, managing patient responses and conducting follow-ups.
Upon receiving a message, the multilingual Link Health team members initiated a conversation with the patient, providing information about Lifeline, gauging their interest, and guiding them through the digital enrollment process. The Link Health digital navigators shared an abbreviated digital sign-up form via text, which patients completed from their personal devices, and their information was uploaded to a HIPAA-compliant Google Firebase dashboard. Finally, the Link Health team reviewed dashboard entries and sent formal applications for the Lifeline program. After the patient’s application was approved, the team texted patients their login credentials and unique password generated by the federal government as an access code to officially enroll in Lifeline. Patients were considered to be “helped to enroll” if their information was successfully uploaded into the Firebase dashboard and a follow-up message was sent to the patient with their Lifeline login information and access code. Demographic- (racial, language, gender, and age), qualification method-, and timeline-data from the dashboard were collected by Link Health and provided to the authors in anonymized form. Results were then synthesized using Google Sheets.
RESULTS
Across 6 months of text-campaigns, clinic partners reached approximately 68,529 patients with information about the Lifeline program. Among all patients reached, 2.15% (n=1,470) were assisted in completing an application for Lifeline.
Figure 1: A largely Hispanic/Latino population was assisted in signing up for Lifeline.
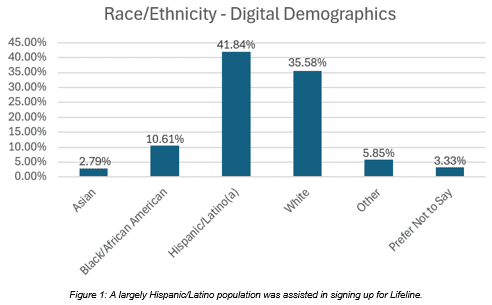
Figure 1 A largely Hispanic/Latino population was assisted in signing up for Lifeline.
2.79% (n=41) self-identified as Asian, 10.61% (n=156) as Black/African-American, 41.84% (n=615) as Hispanic, 35.58% (n=523) as White, 5.85% (n=86) as Other, and 3.33% (n=49) preferred not to say.
Figure 2: A largely English-speaking, but sizeable Spanish-speaking, population was assisted in signing up for Lifeline.
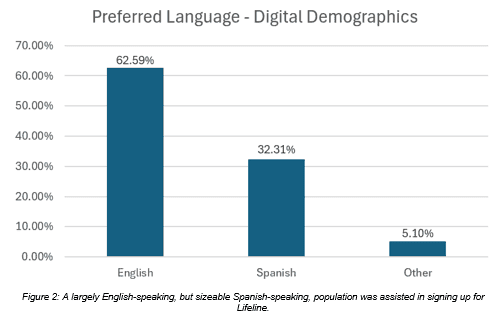
Figure 2 A largely English-speaking, but sizeable Spanish-speaking, population was assisted in signing up for Lifeline.
Additionally, among primary/preferred languages, 62.59% (n=920) preferred English, 32.31% (n=475) preferred Spanish, and 5.10% (n=75) preferred another language.
Figure 3: A largely female population was assisted in signing up for Lifeline.
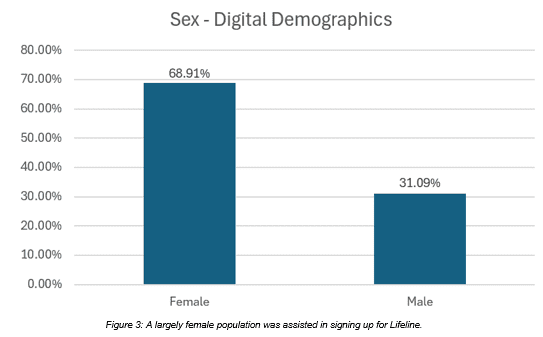
Figure 3 A largely female population was assisted in signing up for Lifeline.
Furthermore, 68.91% (n=1013) of all individuals signing up self-identified as female, and 31.09% (n=457) self-identified as male.
Figure 4: A largely young to middle-aged population was assisted in signing up for Lifeline.
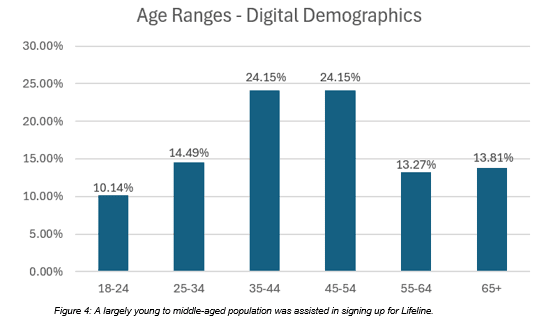
Figure 4 A largely young to middle-aged population was assisted in signing up for Lifeline.
Overall, the population assisted was predominantly composed of young and middle-aged adults, with 10.14% (n=149) between 18-24 years old, 14.49% (n=213) between 25-34, 24.15% (n=355) between 35-44, 24.15% (n=355) between 45-54, 13.27% (n=195) between 55-64, and 13.81% (n=203) aged 65 years or older.
Figure 5: Patients qualified for Lifeline through a number of methods, but the majority qualified via prior enrollment in SNAP.
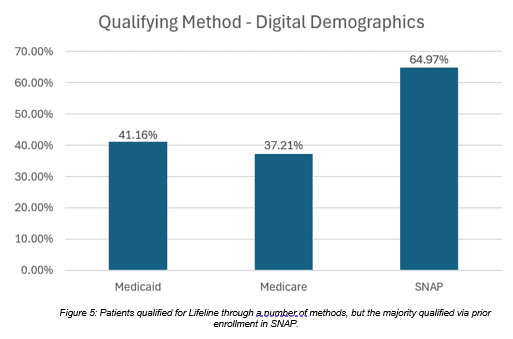
Figure 5 Patients qualified for Lifeline through a number of methods, but the majority qualified via prior enrollment in SNAP.
Patients qualified for the Lifeline program via other benefit programs, with 41.16% (n=605) qualifying through Medicaid, 37.21% (n=547) qualifying through Medicare, and 64.97% (n=955) qualifying through SNAP (totals amount to over 100%, owing to patients being enrolled in multiple programs) (Table 1).
Table 1 Link Health Digital Demographics by Enrollment Method, June 2024-December 2024 (N=1470)
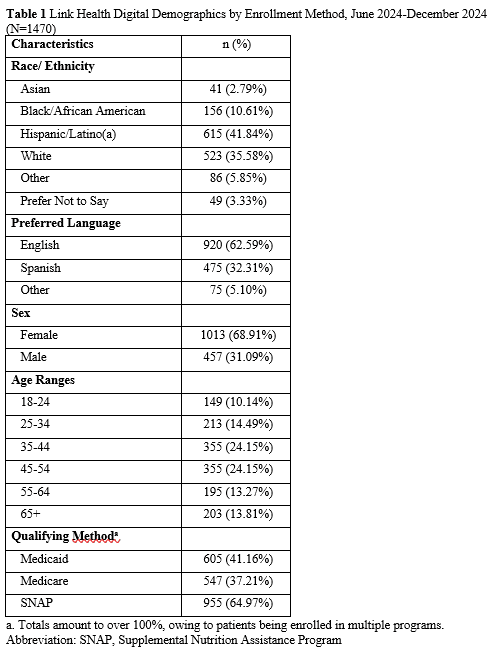
Table 1 Link Health Digital Demographics by Enrollment Method, June 2024-December 2024 (N=1470)
a. Totals amount to over 100%, owing to patients being enrolled in multiple programs.
Abbreviation: SNAP, Supplemental Nutrition Assistance Program
DISCUSSION
Link Health utilized an online text-message platform to engage with communities throughout Massachusetts, reaching nearly 70,000 patients with information about the Lifeline program. To our knowledge, this is the first study to evaluate text-based outreach for Lifeline. Facilitating Lifeline enrollments has allowed Link Health to continue to support patients’ broadband connectivity. The organization’s ability to pivot from enrollments in a similar discount program, the Affordable Connectivity Program (ACP), to Lifeline is encouraging, especially in the wake of the gap left by the ACP’s loss of funding in 2024.[9]Lifeline. (n.d.). Lifeline. Universal Service Administrative Company. https://www.usac.org/lifeline/[10]Federal Communications Commission. (2025). Affordable Connectivity Program. Fcc.gov. https://www.fcc.gov/acp/
Engagement largely occurred within a young to middle-aged adult, female, Hispanic demographic. A large proportion of participants were Spanish speaking. The results suggest text-based enrollment may support individuals across demographic categories. This was likely facilitated through Link Health’s engagement and partnerships with FQHCs, which support patients who may encounter barriers to care, including lack of transportation and under- and uninsured statuses.[11]Nguyen KH, Giron NC, Cole MB. National Prevalence of Social Risk Factors at Federally Qualified Health Centers. JAMA Intern Med. 2024;184(8):980–982. doi:10.1001/jamainternmed.2024.1881 We found that among those who applied for the Lifeline program using Link Health’s platform, nearly 40% preferred to speak a language other than English, suggesting Lifeline enrollment for patients of limited English proficiency may be enhanced via multilingual, digital teams. Spanish-speaking patient navigators may have empowered patients to communicate freely, and facilitated the smooth transfer of information to patients on the importance of the Lifeline program and how to sign up. Additionally, applicants’ diversity in age indicates older adult populations may not be limited by Link Health’s digital intervention. In fact, elderly (65 years and older) individuals accounted for 13.81% of sign-ups. Link Health’s streamlined digital forms likely enabled older adult participation, in spite of potential digital literacy gaps.[12]Finkelstein R, Wu Y, Brennan-Ing M. Older adults' experiences with using information and communication technology and tech support services in New York City: findings and recommendations for post-pandemic digital pedagogy for older adults. Front Psychol. 2023 Apr 17;14:1129512. doi: 10.3389/fpsyg.2023.1129512. PMID: 37138998; PMCID: PMC10150999.
Additionally, patients qualified for Lifeline in a number of ways. Nearly 64.97% of all patients qualified for Lifeline as current SNAP-enrollees, 37.21% as current Medicare-enrollees, and 41.16% as current Medicaid-enrollees, with the vast majority of patients already enrolled in at least one program (65.78%). These findings suggest an overlap between broadband insecurity, food insecurity, and public insurance coverage. However, because this analysis reflects those who enrolled, it may not fully capture individuals with broadband insecurity who did not respond or did not qualify through other programs.
Inequitable access to broadband services remains an ongoing challenge in Link Health’s service areas. Prior research indicates that Hispanic- and Black-majority neighborhoods in Boston face roughly double the rates of broadband insecurity compared to White-majority neighborhoods.[13]Li, Y., Spoer, B. R., Lampe, T. M., Hsieh, P., Nelson, I. S., A. Vierse, et al. (2023). Racial/ethnic and income disparities in neighborhood-level broadband access in 905 US cities, 2017–2021. Public Health, 217, 205–211. https://doi.org/10.1016/j.puhe.2023.02.001 Link Health is making an effort to address these insecurities, and the relatively high proportion of Hispanic enrollees (41.8%) reflects these disparities. However, only roughly a tenth of the patients enrolled by Link Health were Black/African-American, suggesting room for improvement in outreach to this group. Overall, these data suggest partnered-outreach with CHCs can mitigate inequities noted in federal reports.[14]van Kessel, R., Wong, B. L. H., Clemens, T., & Brand, H. (2022). Digital health literacy as a super determinant of health: More than simply the sum of its parts. Internet Interventions, 27(27), 100500. https://doi.org/10.1016/j.invent.2022.100500[15]Viveros-Uehara, T. (2021). Boston Human Rights Commission Broadband Access in Boston Project Report. https://www.boston.gov/sites/default/files/file/2022/07/Broadband-Access%20Spring%202021.pdf Importantly, those that Link Health reached represented diverse individuals, meeting the unique needs of Boston’s populace and working to address racial inequities in internet access. While this study does present an approach that may be suitable for the Greater Boston population, with a focus on Spanish- and English-speaking patients, it is important to recognize that the approach outlined here may fall short in other metroplexes with different demographics. Thus, we recommend that future pilots be conducted into text-based digital campaigns for Lifeline sign-ups in more diverse geographic and linguistic contexts.
Additionally, the 2.15% response rate is comparatively similar to other text campaigns aimed at enrolling patients in government benefits programs. In another campaign by BDT, focusing on helping patients from Colorado, Massachusetts, Montana, and Virginia recertify their enrollment in WIC, approximately 6%, 4%, 6%, and 9%, respectively, of those receiving texts requested a certification appointment, a key step towards the recertification process.[6]Center on Budget and Policy Priorities & Benefits Data Trust. (2022). Maximizing WIC participation with text messaging: A guide for WIC agencies. Digital Government Hub. https://digitalgovernmenthub.org/wp-content/uploads/2022/07/cbpp-bdt-wic-texting-guide.pdf This campaign benefits from focusing on re-enrolling patients into programs they are already familiar with, whereas Lifeline outreach focused entirely on patients who have not had prior enrollment in the program. Additionally, the U.S. General Services Administration, which collaborated with the city of Norfolk, Virginia’s Department of Human Services to remind families to renew their Medicaid, encountered barriers to outreach. Specifically, they identified that Medicaid enrollees expressed skepticism regarding the text messages they received and that many others did not read the messages.[16]General Services Administration. (2024, December 17). Making government text messaging more effective with Notify.gov. https://www.gsa.gov/blog/2024/12/17/making-government-text-messaging-more-effective-with-notifygov In context, the Lifeline campaign may have encountered similar issues, with patients either expressing hesitancy engaging in a sensitive matter such as benefit enrollment with an unknown individual or having missed the message entirely. Utilizing a warm handoff of the patient between the clinic and the Link Health team was designed to reduce feelings of uncertainty in engaging with Link Health, and follow-up messages to patients who failed to respond after initial conversations were integrated into the outreach process to avoid having patients miss the messages. However, in the future, campaigns may find greater success by maintaining the warm handoff of the patient by having the clinic send periodic check-in messages to patients from the clinic’s number (a number the patients may recognize based on prior text reminders regarding regular appointments and other communication), in addition to the follow-ups from the Link Health team. In pursuing a dual follow-up outreach method, patients may express greater trust of Link Health’s services, and messages may be less likely to be ignored as spam. Another possible limitation to this study is the lack of a control group used to assess enrollment in Lifeline. Future studies may consider engaging in a quasi-experimental designed study and comparing Lifeline enrollment and internet connectivity outcomes after the study’s conclusion.
Finally, it should be noted that the intervention model identified by Link Health is largely affordable. Text messages cost as little as 1 cent per message (for short, text-only messages under 150 characters) and 2.5 cents per message (for long MMS messages). For some patients, it takes as few as four messages to help them enroll in Lifeline. This means enrolling patients in a benefit that saves them $111 per year can cost less than ten cents, highlighting the feasibility of implementation for cost-pressed healthcare organizations and systems.
CONCLUSION
Digital literacy and internet connectivity have been called a “super social determinant of health,” referring to their impact on the promotion of skills development, on increasing access to vital resources (including government assistance safety-net programs), and on connectedness with others.[17]Prewitt, E., Namita Seth Mohta, Gordon, L., & Lee, T. H. (2025). Digital Care Is Health Care. NEJM Catalyst, 6(3). https://doi.org/10.1056/cat.25.0057[18]Sieck, C. J., Sheon, A., Ancker, J. S., Castek, J., Callahan, B., & Siefer, A. (2021). Digital inclusion as a social determinant of health. NPJ Digital Medicine, 4(1). https://doi.org/10.1038/s41746-021-00413-8 We contend that digital access interacts with many key SDOH, including educational, employment, and access to care. Hence, Link Health’s efforts to enroll disadvantaged patients in the Lifeline program targets a critical health determinant. Ultimately, text-based outreach enables broad reach in capturing large numbers of patients—yet, there is still a limited focus on text-campaigns aimed at increasing enrollment in federal benefit programs. By leveraging mobile technology, these campaigns overcome traditional barriers to communication, such as the inefficiencies of paper mail and the absence of real-time feedback and support, and ensure timely delivery of critical updates to beneficiaries. Our findings suggest text-messaging platforms are effective in addressing these challenges, thus providing a pathway for individuals to access essential services like subsidized internet and phone connectivity.
Link Health’s text-based outreach adds to its robust non text-based interventions, which involves weekly in-person outreach at FQHCs in Boston and Houston that have resulted in approximately 1,700 patients signing up for nearly 2,300 programs. During Link Health’s most recent Patient Navigator cohort, Navigators engaged with (greeted and discussed Link Health with) an estimated 10-15 patients per clinic, resulting in an average of 3.2 patients signing up for (i.e., completed an application form for) 4.5 programs per clinic. The number of program sign-ups per patient engaged is high in the in-person setting by comparison to the text outreach conducted in this study. However, text-outreach substantially increases the number of patients that can be engaged within a short time frame and over a larger distance.
The evidence supporting Link Health's intervention model is substantial. Since its establishment in 2022, the organization has reached over 120,000 individuals through digital, text-based outreach, resulting in successful program enrollment-assistance for 3,000+ beneficiaries. These efforts have facilitated the distribution of over $4,000,000 in financial assistance across 10 federal programs, including Lifeline. Link Health’s success through the digital, text-based intervention model demonstrates the viability of integrating benefits enrollment within healthcare systems and highlights its potential for broader implementation across diverse clinical settings.
Declarations
Ethics approval and consent to participate
The manuscript reports that the Northeastern Institutional Review Board determined this secondary analysis of operational data fell outside the definition of human-subjects research and required no additional IRB approval.
Consent for publication
Not applicable.
Availability of data and materials
The operational enrollment data analyzed in this article are not publicly available. De-identified summary data may be available from the corresponding author on reasonable request, subject to applicable privacy and institutional constraints.
Competing interests
The authors declare no commercial or financial conflict of interest.
Funding
No funding was received for this research.
Authors' contributions
Abhi Jain: Writing - original draft; Writing - review and editing; Conceptualization; Investigation; Software; Data curation; Methodology; Supervision; Formal analysis; Project administration; Validation; Resources; Visualization | Timothy Scheinert: Writing - original draft; Writing - review and editing; Conceptualization; Investigation; Methodology; Supervision; Formal analysis; Project administration; Validation; Resources | Sammer Marzouk: Writing - original draft; Writing - review and editing; Conceptualization; Investigation | Alessandro Hammond: Writing - original draft; Writing - review and editing; Conceptualization; Investigation | Steven Lauterwasser: Writing - original draft; Writing - review and editing; Conceptualization; Validation; Visualization; Formal analysis; Investigation | Alister Martin: Writing - original draft; Writing - review and editing; Conceptualization; Investigation; Software; Data curation; Project administration; Validation; Supervision; Funding acquisition
REFERENCES
- Headrick, G., Ruth, A., White, S. A., Ellison, C., Seligman, H., Bleich, S. N., et al. (2022). Integration and coordination across public benefit programs: Insights from state and local government leaders in the United States. Preventive medicine reports, 31, 102077. https://doi.org/10.1016/j.pmedr.2022.102077
- Federal Communications Commission. (2012, January 27). Lifeline Program for Low-Income Consumers. Federal Communications Commission. https://www.fcc.gov/general/lifeline-program-low-income-consumers
- Jones, C. H., & Dolsten, M. (2024). Healthcare on the brink: navigating the challenges of an aging society in the United States. Npj Aging, 10(1), 1–10. https://doi.org/10.1038/s41514-024-00148-2
- Lim, H. A., Lee, J. S. W., Lim, M. H., Teo, L. P. Z., Sin, N. S. W., Lim, R. W., et al. (2022). Bridging Connectivity Issues in Digital Access and Literacy: Reflections on Empowering Vulnerable Older Adults in Singapore. JMIR Aging, 5(2), e34764. https://doi.org/10.2196/34764
- Health Law Lab. (2021). Text message outreach to support SNAP and WIC enrollment in California. Retrieved November 19, 2024, from https://www.healthlawlab.org/wp-content/uploads/2021/10/Text-Message-Outreach-to-Support-SNAP-and-WIC-Enrollment-2021.pdf
- Center on Budget and Policy Priorities & Benefits Data Trust. (2022). Maximizing WIC participation with text messaging: A guide for WIC agencies. Digital Government Hub. https://digitalgovernmenthub.org/wp-content/uploads/2022/07/cbpp-bdt-wic-texting-guide.pdf
- Code for America. (2024, December 17). Simplifying Communications to Help People Maintain Benefits in Louisiana — Code for America. Code for America. https://codeforamerica.org/success-stories/simplifying-communications-to-help-people-maintain-benefits-in-louisiana/
- Joseph, N. P., Hider, A. M., Contreras, D., Velasquez, D. E., & Martin, A. (2023). Bridging the digital divide through on-site, health center-based internet clinics. NEJM Catalyst. https://doi.org/10.1056/CAT.23.0099
- Lifeline. (n.d.). Lifeline. Universal Service Administrative Company. https://www.usac.org/lifeline/
- Federal Communications Commission. (2025). Affordable Connectivity Program. Fcc.gov. https://www.fcc.gov/acp/
- Nguyen KH, Giron NC, Cole MB. National Prevalence of Social Risk Factors at Federally Qualified Health Centers. JAMA Intern Med. 2024;184(8):980–982. doi:10.1001/jamainternmed.2024.1881
- Finkelstein R, Wu Y, Brennan-Ing M. Older adults' experiences with using information and communication technology and tech support services in New York City: findings and recommendations for post-pandemic digital pedagogy for older adults. Front Psychol. 2023 Apr 17;14:1129512. doi: 10.3389/fpsyg.2023.1129512. PMID: 37138998; PMCID: PMC10150999.
- Li, Y., Spoer, B. R., Lampe, T. M., Hsieh, P., Nelson, I. S., A. Vierse, et al. (2023). Racial/ethnic and income disparities in neighborhood-level broadband access in 905 US cities, 2017–2021. Public Health, 217, 205–211. https://doi.org/10.1016/j.puhe.2023.02.001
- van Kessel, R., Wong, B. L. H., Clemens, T., & Brand, H. (2022). Digital health literacy as a super determinant of health: More than simply the sum of its parts. Internet Interventions, 27(27), 100500. https://doi.org/10.1016/j.invent.2022.100500
- Viveros-Uehara, T. (2021). Boston Human Rights Commission Broadband Access in Boston Project Report. https://www.boston.gov/sites/default/files/file/2022/07/Broadband-Access%20Spring%202021.pdf
- General Services Administration. (2024, December 17). Making government text messaging more effective with Notify.gov. https://www.gsa.gov/blog/2024/12/17/making-government-text-messaging-more-effective-with-notifygov
- Prewitt, E., Namita Seth Mohta, Gordon, L., & Lee, T. H. (2025). Digital Care Is Health Care. NEJM Catalyst, 6(3). https://doi.org/10.1056/cat.25.0057
- Sieck, C. J., Sheon, A., Ancker, J. S., Castek, J., Callahan, B., & Siefer, A. (2021). Digital inclusion as a social determinant of health. NPJ Digital Medicine, 4(1). https://doi.org/10.1038/s41746-021-00413-8