

Abstract:
Background
Remote Patient Monitoring (RPM) has emerged as a promising approach to managing chronic conditions such as asthma, particularly during the COVID-19 pandemic. However, limited research exists on the use of qualitative analysis to capture patient feedback and experiences in RPM programs. This study builds upon a quantitative observational study that explored the impact of RPM on patients with moderate to severe asthma.
Objective
This study aimed to evaluate the feasibility and usability of Keva365 and to explore its impact on patient-provider relationships, asthma management, patient compliance, and engagement.
Methods
A purposeful sample of six patients with moderate to severe persistent asthma participated in the study. Over a nine-month period, participants were interviewed once using an open-ended question guide to collect qualitative data. The interviews were recorded, transcribed, and analyzed thematically using NVivo software. Data were used to assess the feasibility, usability, and impact of the RPM intervention on patient experiences. Written consent to publish these details has been obtained from all participants who were included in this research.
Results
Thematic analysis identified key themes related to patients' experiences with the app, their compliance and engagement with the program, their relationships with providers, and asthma management. All participants reported positive experiences with the program, noting the app’s usability, efficiency, and impact on their relationships with healthcare providers. Participants expressed high levels of satisfaction and a willingness to recommend the program to others. Feedback from the interviews contributed to near real-time modifications of the RPM application, enhancing its usability and navigation.
Conclusions
The study found that integrating patient feedback is essential for improving the usability of RPM platforms. Continuous iterative refinement based on patient experiences can lead to more patient-centered digital health solutions, enhancing both patient compliance and the overall care experience. The findings suggest that RPM programs can effectively support asthma management while fostering positive patient-provider relationships.
Keywords
Remote Patient Monitoring, Asthma, Qualitative Research, Patient Feedback, Usability, Compliance, Patient Engagement
Introduction
Due to rising patient volumes in pulmonology clinics, accessing timely, hands-on care has become increasingly challenging [1]Reid, D.M., Mehta, J., Mehta, S., Divgi, V.D. and Anis, K.H. (2022) ‘Clinically meaningful data from remote spirometry monitoring in asthma management in a US-based observational study’, Chest, 162(4), p. A2474. doi:10.1016/j.chest.2022.08.2026. Available at: https://doi.org/10.1016/j.chest.2022.08.2026 (Accessed: 15 September 2025)., [2]Serrano, L.P., Maita, K.C., Avila, F.R., Torres-Guzman, R.A., Garcia, J.P., Eldaly, A.S., Haider, C.R., Felton, C.L., Paulson, M.R., Maniaci, M.J. and Forte, A.J. (2023) ‘Benefits and challenges of remote patient monitoring as perceived by health care practitioners: A systematic review’, The Permanente Journal, 27(4), pp. 100–111. doi:10.7812/TPP/23.022. Available at: https://doi.org/10.7812/TPP/23.022 (Accessed: 15 September 2025).. Patients with chronic asthma have reported that self-managing their illness feels isolating and overwhelming [3]Farnesi, B.C., Ducharme, F.M., Blais, L., Collin, J., Lavoie, K.L., Bacon, S.L., McKinney, M.L. and Peláez, S. (2019) ‘Guided asthma self-management or patient self-adjustment? Using patients’ narratives to better understand adherence to asthma treatment’, Patient Preference and Adherence, 13, pp. 587–597. doi:10.2147/PPA.S195585. Available at: https://doi.org/10.2147/PPA.S195585 (Accessed: 15 September 2025).. These findings suggest that support from a clinical team and access to preventive care are not only pertinent but essential as patient populations continue to grow. However, the combined effects of the COVID-19 pandemic, staffing shortages, and restrictions on in-person visits have limited the ability of clinical teams to adequately meet the needs of patients with asthma [4]Shah, S.A., Quint, J.K. and Sheikh, A. (2022) ‘Impact of COVID-19 pandemic on asthma exacerbations: Retrospective cohort study of over 500,000 patients in a national English primary care database’, The Lancet Regional Health – Europe, 19, 100428. doi:10.1016/j.lanepe.2022.100428. (Accessed: 15 September 2025)., [5]Philip, K.E.J., Buttery, S., Williams, P., Vijayakumar, B., Tonkin, J., Cumella, A., Renwick, L., Ogden, L., Quint, J.K., Johnston, S.L., Polkey, M.I. and Hopkinson, N.S. (2022) ‘Impact of COVID-19 on people with asthma: A mixed methods analysis from a UK-wide survey’, BMJ Open Respiratory Research, 9(1), e001056. doi:10.1136/bmjresp-2021-001056. Available at: https://bmjopenrespres.bmj.com/content/9/1/e001056 (Accessed: 15 September 2025).. In response, the use of telemedicine and telehealth services expanded significantly, with increased adoption of remote patient care technologies such as Remote Patient Monitoring (RPM) during the pandemic [6]Ogden, L., Quint, J.K., Johnston, S.L., Polkey, M.I. and Hopkinson, N.S. (2022) ‘Impact of COVID-19 on people with asthma: A mixed methods analysis from a UK-wide survey’, BMJ Open Respiratory Research, 9(1), e001056. doi:10.1136/bmjresp-2021-001056. Available at: https://bmjopenrespres.bmj.com/content/9/1/e001056 (Accessed: 15 September 2025).. RPM is broadly defined as a technology that enables monitoring of patients outside conventional clinical settings, such as in the home or other remote locations [6]Ogden, L., Quint, J.K., Johnston, S.L., Polkey, M.I. and Hopkinson, N.S. (2022) ‘Impact of COVID-19 on people with asthma: A mixed methods analysis from a UK-wide survey’, BMJ Open Respiratory Research, 9(1), e001056. doi:10.1136/bmjresp-2021-001056. Available at: https://bmjopenrespres.bmj.com/content/9/1/e001056 (Accessed: 15 September 2025).. Studies on RPM suggest that it offers an economic, time-efficient, and practical option for patients [7]Hyder, M. and Razzak, J. (2020) ‘Telemedicine in the United States: An introduction for students and residents’, Journal of Medical Internet Research, 22(11), e20839. doi:10.2196/20839. Available at: https://www.jmir.org/2020/11/e20839(Accessed: 15 September 2025)..
In 2021, the Centers for Disease Control and Prevention (CDC) reported that the prevalence of asthma attacks among adults and children with current asthma was 39.4% [8]Reid, D., Mehta, J., Anis, K. and Mehta, S. (2023) ‘Impact of remote patient monitoring platform on patients with moderate to severe persistent asthma: Observational study’, JMIR Formative Research, 7, e51065. doi:10.2196/51065. Available at: https://formative.jmir.org/2023/1/e51065 (Accessed: 15 September 2025)., [9]Centers for Disease Control and Prevention (2023) Asthma surveillance in the U.S., 2001–2021. Atlanta, GA: Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/asthma/asthma-prevalence-us-2023-508.pdf(Accessed: 15 September 2025)., [10]Centers for Disease Control and Prevention (2023) Most recent national asthma data. Atlanta, GA: Centers for Disease Control and Prevention. Updated 17 June 2024. Available at: https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm (Accessed: 15 September 2025).. Studies further indicate that, regardless of cause, exacerbation rates were substantially lower during 2020–2021 compared with 2016–2019, coinciding with the introduction of Remote Patient Monitoring (RPM) tools into patient care plans [11]Miller, R.L., Breysse, P.N., Jacobs, D.E., Kanchanaraksa, S., Morley, R.L., Sampson, N.R. and Svendsen, E.R. (2021) ‘Impact of the COVID-19 pandemic on asthma exacerbations in the United States: Insights from electronic health records and remote patient monitoring’, Journal of Allergy and Clinical Immunology: In Practice, 9(8), pp. 2903–2913. doi:10.1016/j.jaip.2021.06.034..
In 2020, there were approximately 908,000 emergency department (ED) visits in the United States with asthma as the primary diagnosis, corresponding to a rate of 29.8 visits per 10,000 population [8]Reid, D., Mehta, J., Anis, K. and Mehta, S. (2023) ‘Impact of remote patient monitoring platform on patients with moderate to severe persistent asthma: Observational study’, JMIR Formative Research, 7, e51065. doi:10.2196/51065. Available at: https://formative.jmir.org/2023/1/e51065 (Accessed: 15 September 2025)., [9]Centers for Disease Control and Prevention (2023) Asthma surveillance in the U.S., 2001–2021. Atlanta, GA: Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/asthma/asthma-prevalence-us-2023-508.pdf(Accessed: 15 September 2025)., [10]Centers for Disease Control and Prevention (2023) Most recent national asthma data. Atlanta, GA: Centers for Disease Control and Prevention. Updated 17 June 2024. Available at: https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm (Accessed: 15 September 2025).. Moreover, in cases of emergencies or exacerbations triggered by COVID-19, access to supportive resources such as telehealth and Remote Patient Monitoring (RPM) has proven especially valuable [8]Reid, D., Mehta, J., Anis, K. and Mehta, S. (2023) ‘Impact of remote patient monitoring platform on patients with moderate to severe persistent asthma: Observational study’, JMIR Formative Research, 7, e51065. doi:10.2196/51065. Available at: https://formative.jmir.org/2023/1/e51065 (Accessed: 15 September 2025)., [9]Centers for Disease Control and Prevention (2023) Asthma surveillance in the U.S., 2001–2021. Atlanta, GA: Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/asthma/asthma-prevalence-us-2023-508.pdf(Accessed: 15 September 2025)., [10]Centers for Disease Control and Prevention (2023) Most recent national asthma data. Atlanta, GA: Centers for Disease Control and Prevention. Updated 17 June 2024. Available at: https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm (Accessed: 15 September 2025)., [12]Coffey, J.D., Christopherson, L.A., Glasgow, A.E., Pearson, K.K., Brown, J.K., Gathje, S.R., Sangaralingham, L.R., Carmona Porquera, E.M., Virk, A., Orenstein, R., Speicher, L.L., Bierle, D.M., Ganesh, R., Cox, D.L., Blegen, R.N. and Haddad, T.C. (2021) ‘Implementation of a multisite, interdisciplinary remote patient monitoring program for ambulatory management of patients with COVID-19’, NPJ Digital Medicine, 4(1), 123. doi:10.1038/s41746-021-00490-9. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC8363637/ (Accessed: 15 September 2025)., [13]Fusi-Schmidhauser, T., Froggatt, K. and Preston, N. (2020) ‘Living with advanced chronic obstructive pulmonary disease: A qualitative interview study with patients and informal carers’, COPD: Journal of Chronic Obstructive Pulmonary Disease, 17(4), pp. 410–418. doi:10.1080/15412555.2020.1782867. Available at: https://doi.org/10.1080/15412555.2020.1782867 (Accessed: 15 September 2025).. The Keva Health Platform is an RPM tool that enables patients to receive care while overcoming barriers such as location, proximity, and time.
Despite its demonstrated effectiveness, RPM tools remain limited, particularly in pulmonology. Research in this area is sparse [14]Delameillieure, A., Dobbels, F., Vandekerkhof, S. et al. (2021) ‘Patients’ and healthcare professionals’ perspectives on the idiopathic pulmonary fibrosis care journey: A qualitative study’, BMC Pulmonary Medicine, 21, 93. doi:10.1186/s12890-021-01431-8. Available at: https://doi.org/10.1186/s12890-021-01431-8 (Accessed: 15 September 2025)., [15]Genberg, E.M., Viitanen, H.T., Mäkelä, M.J. et al. (2023) ‘Impact of a digital web-based asthma platform, a real-life study’, BMC Pulmonary Medicine, 23, 165. doi:10.1186/s12890-023-02467-8. Available at: https://doi.org/10.1186/s12890-023-02467-8 (Accessed: 15 September 2025)., [16]L, S.P., Khurdi, S., G, P.T. and Mary, S.P. (2024) ‘Impact of remote patient monitoring systems on nursing time, healthcare providers, and patient satisfaction in general wards’, Cureus, 16(6), e61646. doi:10.7759/cureus.61646. Available at: https://doi.org/10.7759/cureus.61646 (Accessed: 15 September 2025)., highlighting the need for technologies that strengthen the patient–physician relationship to improve care outcomes [17]Caneiras, C., Jácome, C., Moreira, E., Oliveira, D., Dias, C.C., Mendonça, L., Mayoralas-Alises, S., Fonseca, J.A., Diaz-Lobato, S., Escarrabill, J. and Winck, J.C. (2022) ‘A qualitative study of patient and carer experiences with home respiratory therapies: Long-term oxygen therapy and home mechanical ventilation’, Pulmonology, 28(4), pp. 268–275. doi:10.1016/j.pulmoe.2021.05.010. Available at: https://doi.org/10.1016/j.pulmoe.2021.05.010 (Accessed: 15 September 2025)., [18]American Lung Association (2024) Asthma trends brief: Asthma trends and burden. Chicago, IL: American Lung Association. Available at: https://www.lung.org/research/trends-in-lung-disease/asthma-trends-brief/trends-and-burden(Accessed: 15 September 2025).. While analyses of exacerbation rates, hospital readmissions, costs, and oral corticosteroid prescriptions have provided valuable insights, evaluation from the patient perspective remains limited [15]Genberg, E.M., Viitanen, H.T., Mäkelä, M.J. et al. (2023) ‘Impact of a digital web-based asthma platform, a real-life study’, BMC Pulmonary Medicine, 23, 165. doi:10.1186/s12890-023-02467-8. Available at: https://doi.org/10.1186/s12890-023-02467-8 (Accessed: 15 September 2025)., [16]L, S.P., Khurdi, S., G, P.T. and Mary, S.P. (2024) ‘Impact of remote patient monitoring systems on nursing time, healthcare providers, and patient satisfaction in general wards’, Cureus, 16(6), e61646. doi:10.7759/cureus.61646. Available at: https://doi.org/10.7759/cureus.61646 (Accessed: 15 September 2025).. Although some qualitative studies have explored clinicians’ experiences with RPM—including pulmonologists, pediatricians, physician assistants, and nurses—there is considerably less research examining the patient experience [13]Fusi-Schmidhauser, T., Froggatt, K. and Preston, N. (2020) ‘Living with advanced chronic obstructive pulmonary disease: A qualitative interview study with patients and informal carers’, COPD: Journal of Chronic Obstructive Pulmonary Disease, 17(4), pp. 410–418. doi:10.1080/15412555.2020.1782867. Available at: https://doi.org/10.1080/15412555.2020.1782867 (Accessed: 15 September 2025)., [15]Genberg, E.M., Viitanen, H.T., Mäkelä, M.J. et al. (2023) ‘Impact of a digital web-based asthma platform, a real-life study’, BMC Pulmonary Medicine, 23, 165. doi:10.1186/s12890-023-02467-8. Available at: https://doi.org/10.1186/s12890-023-02467-8 (Accessed: 15 September 2025)., [17]Caneiras, C., Jácome, C., Moreira, E., Oliveira, D., Dias, C.C., Mendonça, L., Mayoralas-Alises, S., Fonseca, J.A., Diaz-Lobato, S., Escarrabill, J. and Winck, J.C. (2022) ‘A qualitative study of patient and carer experiences with home respiratory therapies: Long-term oxygen therapy and home mechanical ventilation’, Pulmonology, 28(4), pp. 268–275. doi:10.1016/j.pulmoe.2021.05.010. Available at: https://doi.org/10.1016/j.pulmoe.2021.05.010 (Accessed: 15 September 2025)., [18]American Lung Association (2024) Asthma trends brief: Asthma trends and burden. Chicago, IL: American Lung Association. Available at: https://www.lung.org/research/trends-in-lung-disease/asthma-trends-brief/trends-and-burden(Accessed: 15 September 2025)., [19]American Medical Association (2024) Remote patient monitoring implementation playbook overview. Chicago, IL: American Medical Association. Available at: https://www.ama-assn.org/practice-management/digital/remote-patient-monitoring-implementation-playbook-overview (Accessed: 15 September 2025).. This study is part of a larger program designed to reduce hospital visits due to asthma exacerbations between clinic visits, thereby lessening the burden on both payers and patients.
The Keva Health Platform
All necessary access permissions and approvals for using the Keva Health Platform (Keva365) were obtained from the owner, Keva Health. Keva365 is a HIPAA-compliant remote care platform designed to collect, monitor, and process patient data through an integrated ecosystem that includes a mobile app (Keva Talk), Bluetooth-connected devices, and a physician dashboard (Figure 1).
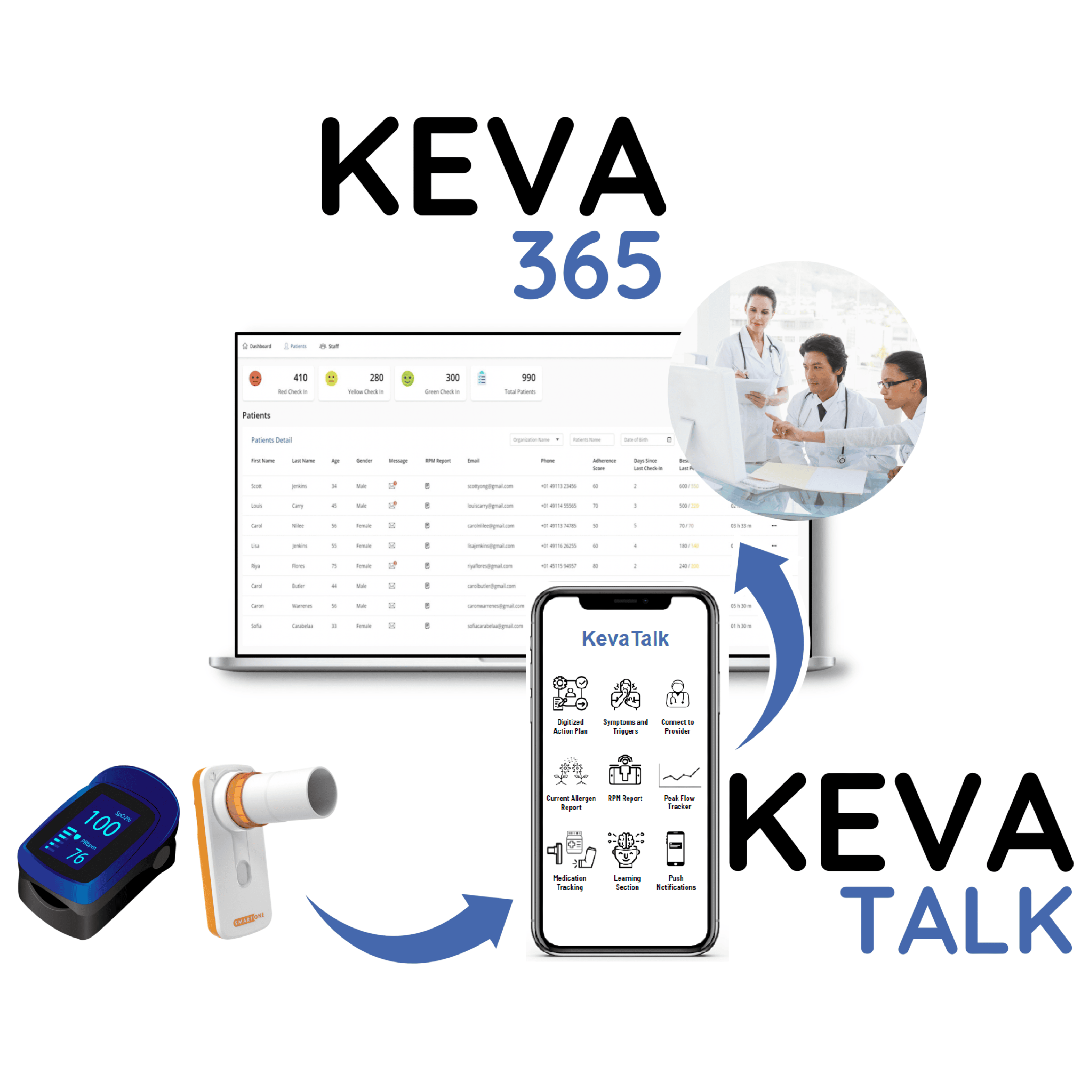
Figure 1: The digital health platform is available on desktop and as an application. The contents of the image are sample (not real) patient data and are for demonstration purposes only. Therefore, does not need to be anonymized.
Figure Legend: The image showcases the Keva365 digital health platform, which features an integrated user interface for both desktop and mobile application access. On the left, the desktop version displays a detailed patient management dashboard, highlighting metrics such as the number of patients and various metrics that are captured remotely. The right side shows the mobile application interface, KevaTalk, designed for efficient communication and streamlined access to essential patient information, including patient check-ins, spirometry readings, oximetry readings, etc.
The platform enables continuous symptom monitoring and generates alerts that are routed to patients or physicians depending on who is responsible for the next clinical action. Patients interact with the system through structured “check-ins,” where they report symptom severity and upload oximetry and spirometry readings. Push notifications encourage adherence by prompting patients to check in multiple times per day.
In addition to daily monitoring, Keva365 offers features that enhance self-management and clinical oversight. These include a digitized action plan, medication reminders, peak flow tracking, and a Current Allergen Report for more detailed symptom reporting. All patient data are curated in the app and synthesized into monthly reports, which the Keva care team uploads directly into the physician’s electronic health record (EHR) system. This ensures providers have access to accurate, longitudinal data that go beyond patient recall during visits, supporting more proactive and informed care.
At-home spirometers were provided to document peak-flow readings that synchronized directly with the mobile application using Bluetooth technology. A respiratory therapist provided training on the use of a spirometer via phone. This was performed during the onboarding process.
Study Objectives
This study is part of a greater longitudinal study aimed to investigate the feasibility and usability of a novel RPM intervention and explore its impact on patient and provider relationships, management of asthma, patient compliance and engagement, and home care for asthma patients during COVID-19. For the purpose of this sub-study, patient experience and feedback were analyzed with the intent to evaluate and refine the Keva Health program.
Methods
Recruitment and Patient Characteristics
The first patient was enrolled in May 2021. The study population consisted of six eligible asthma patients seen in a traditional specialty clinic who consented to participate in this 9-month study. Purposeful sampling was used to recruit participants. Eligible patients were contacted at random by the researchers and invited to participate in a 45-minute interview. The first six patients who agreed formed the interview cohort. All participants completed the interview process in its entirety. This subset was part of a larger 25-person longitudinal study.
Inclusion criteria included moderate to severe asthma and enrollment in the Keva Health program for at least six months. Patients were compensated with a $15 cash card for their participation. Site approval and informed consent were obtained from all participants. Baseline characteristics of the participants are presented in Table 1.
Table 1: Represents the Baseline Characteristics of the participants (n =6)
Variable(s) |
Patients |
|
Age (years) |
Range |
49, 51, 63, 69, 69, 72 |
Gender |
n |
5 (F), 1 (M) |
ATAQ Score* |
Mean (SD) |
1.5 (0.55) |
Asthma Duration (years) |
Approximate Timeline |
9+ years (n=3); 3+ years (n=2); 26+ years (n=1) |
*The Asthma Therapy Assessment Questionnaire (ATAQ) is a validated tool used to assess asthma control and treatment effectiveness. It consists of a series of questions that evaluate the symptoms, medication use, and impact of asthma on daily activities. The ATAQ scores range from 0 to 9, with higher scores indicating poorer asthma control.
Study Design
An interview guide with open-ended questions was developed to facilitate discussion and allow patients to provide spontaneous feedback, capturing the feasibility, usefulness, and perceived importance of functions within the application. The interviewer, who had extensive experience in qualitative interviewing, and her research associate conducted mock interviews with each other for training purposes and to ensure smooth conversational flow. The interview guide was reviewed by the medical director at the clinical site (see Appendix 1).
Interviews were conducted via audio and video, recorded after obtaining participant consent, and lasted between 30 and 60 minutes. All interviews were manually transcribed by the researchers and reviewed three times for accuracy. Transcripts were then analyzed to conduct a thematic analysis [20]Jackson, K. and Bazeley, P. (2019) Qualitative data analysis with NVivo. 3rd edn. Thousand Oaks, CA: Sage. Available at: https://us.sagepub.com/sites/default/files/upm-assets/114916_book_item_114916.pdf (Accessed: 15 September 2025)., [21]Jackson, K. and Bazeley, P. (2019) Qualitative data analysis with NVivo. 3rd edn. Thousand Oaks, CA: Sage. Available at: https://us.sagepub.com/sites/default/files/upm-assets/114916_book_item_114916.pdf (Accessed: 15 September 2025).. NVivo software was used for initial coding, followed by line-by-line coding [20]Jackson, K. and Bazeley, P. (2019) Qualitative data analysis with NVivo. 3rd edn. Thousand Oaks, CA: Sage. Available at: https://us.sagepub.com/sites/default/files/upm-assets/114916_book_item_114916.pdf (Accessed: 15 September 2025)., [21]Jackson, K. and Bazeley, P. (2019) Qualitative data analysis with NVivo. 3rd edn. Thousand Oaks, CA: Sage. Available at: https://us.sagepub.com/sites/default/files/upm-assets/114916_book_item_114916.pdf (Accessed: 15 September 2025).. The sample size was limited to six participants due to resource and time constraints. The study purpose was clearly explained to all participants during recruitment and remained consistent throughout the study.
Data Analysis
Following transcription, the documents were imported into NVivo, where participant feedback on open-ended questions was coded into 24 sub-themes, which were then organized into five main themes (see Table 2). Each time a theme or sub-theme was identified in the text, it was coded accordingly. Table 2 displays both the number of participants who mentioned each theme and the frequency of mentions. Themes with higher frequency scores were considered highly relevant, provided the context indicated significance, importance, or impact on the participant.
Inductive coding and an open-ended style of questioning were chosen to allow authentic, emergent themes without directing or prompting participants. To reduce bias, the researchers who conducted the interviews did not analyze the transcripts. Analysts were blinded to the nature of the interactions and participant identities to minimize confirmation or interaction biases. All themes were reviewed by a clinician to ensure compliance with HIPAA.
In addition to qualitative data, objective platform engagement metrics were collected, including the number of patients who engaged with the app, the percentage of patients completing a validated asthma questionnaire, the number of provider logins, and the duration of use by physicians and nurses.
Table 2: Represents the Most Prominent Themes Emerging from patient interviews.
Themes |
Patient Compliance and Engagement with the Platform |
Impact on Patient-Provider Relationship |
Impact on Managing Asthma |
Impact of Comorbidities on Asthma |
User Experience with the Technology and Devices |
Number1 |
6 |
6 |
6 |
6 |
6 |
Frequency of Mention2 |
30 |
25 |
25 |
6 |
119 |
Number 1, of participants who referred to the theme (Number); Frequency of Mention, of times the theme was mentioned (Frequency)
Table 3: Detailed description of identified sub-themes
Theme 13: Patient Compliance and Engagement with the Platform |
|||||||||
Sub-Themes4 |
Continued usage after the study |
Helpful interaction with the Keva Health Care Team |
Regular Use of the App |
Helpful reminder notification feature |
Not Helpful reminder notifications |
User Referral to Family/Friends |
|||
Number5 |
6 |
5 |
4 |
5 |
1 |
6 |
|||
Frequency of Mention6 |
6 |
5 |
6 |
6 |
1 |
6 |
|||
Theme 2: Impact on Patient-Provider Relationship |
|||||||||
Sub-Themes |
Preference for Clinic Visits over application check-ins |
Preference for application check-ins over Clinic Visits |
Enhanced Patient-Provider Relationship |
Helpful ‘Tracking’ feature between clinic visits |
|||||
Number |
2 |
1 |
6 |
5 |
|||||
Frequency of Mention |
2 |
2 |
12 |
9 |
|||||
Theme 3: Impact on Managing Asthma |
|||||||||
Sub-Themes |
Aids in Asthma Management |
Managing it Alone |
Struggles with Asthma Management before RPM tool intervention |
||||||
Number |
6 |
4 |
5 |
||||||
Frequency of Mention |
8 |
7 |
10 |
||||||
Theme 4: Impact of comorbidities on Asthma |
|||||||||
Sub-Themes |
Comorbidities-impacted Asthma |
Comorbidities Did Not Impact Asthma |
|||||||
Number |
4 |
2 |
|||||||
Frequency of Mention |
4 |
2 |
|||||||
Theme 5: User Experience with the Technology and Devices |
|||||||||
Sub-Themes |
Action Plan Is Set Up |
Action Plan Not Set Up |
Better Technology |
Low Confidence in Spirometry Readings |
Confidence in Spirometry Readings |
User Friendly |
Challenges with App Features |
Helpful App Features |
High User Satisfaction |
Number |
2 |
1 |
1 |
1 |
4 |
6 |
5 |
6 |
6 |
Frequency of Mention |
3 |
2 |
1 |
1 |
4 |
32 |
22 |
39 |
11 |
The five main themes (Theme 1–5) are bolded and numbered at the top of each section. Italicized Sub-Themes 4 are listed under each main theme in separate columns. Number 5 indicates how many participants referred to each theme, and Frequency of Mention 6 reflects how many times the theme was referenced in total. The coding approach combined inductive and deductive thematic analyses: sub-themes were inductively derived from the data, while main themes were developed deductively based on the study framework.
Results
User Experience with the Technology and Devices
Participants generally reported positive experiences with the application and its core features, including the Action Plan, Learn Feature, At-home Spirometry, Medication Feature, and Tracking Tools. Four of six patients expressed confidence in their at-home spirometry readings, which were successfully transmitted to their physician.
All participants found the app intuitive and easy to navigate. Onboarding materials—including a training video, an introductory session with a respiratory therapist, and a brochure—were highlighted as helpful (Female, 69). Representative quotes included, “Right now, to be honest with you, it [the spirometer] was so easy I don’t even remember” (Male, 72) and “It’s user friendly…At first, I thought, oh, my gosh, this is quite a project. But then she says no… it flows right along. Nothing hard about it” (Female, 63).
Several participants noted areas for improvement, such as reminder timing preferences, gaps in certain features, and inconsistencies in Action Plan setup. Patients also suggested enhancements like customizable reminders, color-coding for check-ins, and simplified medication entry aligned with treatment plans. This feedback was subsequently incorporated into updates to the application.
Patient Compliance and Engagement with the Platform
All participants indicated they would continue using the application and would recommend it to others. They reported improved insight into their condition and found the platform easy to navigate. One patient noted, “I think that it's always good when you have more knowledge…Even for people who are not very tech savvy with the training and staff, I think it'd be easy enough for everybody to use” (Female, 51). Five participants highlighted the supportive role of the Keva Health Team, particularly during initial onboarding, and appreciated features such as reminder notifications and medication tracking. Four of six patients used the app at least daily.
Impact on Patient-Provider Relationship
All patients reported that the platform strengthened trust and communication with their providers. They valued the tracking feature for providing day-to-day reports on symptoms and vitals, which facilitated more informed discussions during appointments. One participant explained, “I felt like I did not have to remember…these days, whatever was my trigger. It just helps to track it better, and to give him the information that I do not have to try to remember” (Male, 72). Two patients preferred remote monitoring for routine check-ins, citing convenience and reduced need for in-person visits.
Impact on Managing Asthma
Patients described asthma as a debilitating condition that limited daily activities. Four participants reported managing their asthma largely alone before using the platform, often feeling helpless or isolated. One participant shared, “I would just try to manage it on my own…until I reach a point where… I actually go and ask for help” (Female, 49). The application supported self-management by improving adherence and symptom awareness; one patient noted, “The reminders helped me stay consistent with my inhaler” (Female, 63). Some suggested enhancements, such as flexible reminder timing and streamlined action plan setup.
Impact of Comorbidities
Four participants indicated that comorbidities, including COVID-19, affected their asthma, either through medication side effects or symptom relapses. One stated, “Stress and anxiety caused by medication…whenever I have anxiety or stress I wheeze; it's directly related to my asthma” (Female, 63). Two patients reported no impact from comorbidities.
Discussion
“User experience” with the novel technology emerged as the most frequently mentioned theme. Patients reported positive interactions with the platform, particularly the Action Plan feature when pre-configured by their physicians, which supported adherence to treatment plans. Four of six participants expressed confidence in at-home spirometry, and all participants found the app intuitive. They highlighted features such as symptom tracking, check-ins, the Action Plan, medication tracking, the “Learn” module, reminder notifications, and integrated spirometry and oximetry as particularly helpful.
However, inconsistencies were noted in Action Plan implementation: it was confirmed as set up in two cases, absent in one, and unclear in the remaining three. Despite this, all participants reported that the platform improved patient-provider communication between visits, with five of six emphasizing the value of tracking and check-in features for maintaining a shared daily symptom record.
These findings underscore the importance of iterative, patient-centered technology design. While usability and feature utility contributed to positive experiences, the prominence of user experience–related feedback may reflect the novelty of the intervention rather than sustained clinical impact. New tools often generate heightened engagement, particularly compared with traditional asthma care models. Incorporating patient insights into ongoing development can help address implementation gaps, such as inconsistent Action Plan setup, and improve training, onboarding, and long-term adoption. Future longitudinal research is needed to distinguish short-term enthusiasm from lasting improvements in self-management, clinical outcomes, and care coordination.
Limitations, Implications, and Future Research
This study is limited by its small sample size and gender imbalance, with five female participants and only one male. Such disparity may reflect gendered patterns in digital health adoption and healthcare engagement, but it also introduces potential bias and limits generalizability. Additionally, the first-come basis of participant selection may have captured a sample of more motivated or technologically confident individuals, potentially introducing self-selection bias. Consequently, perspectives from patients who are less digitally literate, less enthusiastic, or more skeptical of remote monitoring technologies may be underrepresented.
Future research would benefit from stratified purposive sampling to include a broader range of patient experiences across digital comfort levels, age, socioeconomic status, and disease severity. Longer study periods, with interviews at multiple intervals (e.g., six months, one year, two years), could provide a more dynamic understanding of patient experiences and platform impact over time.
As with many qualitative studies, findings are based on self-reported data, which may be subject to recall bias, social desirability bias, and subjective interpretation. Despite these limitations, this study provides critical groundwork for patient-centered digital health interventions in asthma management.
With the rise of remote patient monitoring (RPM) technologies, there is increasing potential to extend care to individuals facing geographic, physical, or systemic barriers. When integrated into standard care pathways, RPM may reduce economic burdens on payers while serving as a preventative tool for patients with chronic conditions such as asthma. Thematic analysis, as demonstrated in this study, enables collection of meaningful, patient-reported insights to inform the development of more responsive and effective digital therapeutic platforms [13]Fusi-Schmidhauser, T., Froggatt, K. and Preston, N. (2020) ‘Living with advanced chronic obstructive pulmonary disease: A qualitative interview study with patients and informal carers’, COPD: Journal of Chronic Obstructive Pulmonary Disease, 17(4), pp. 410–418. doi:10.1080/15412555.2020.1782867. Available at: https://doi.org/10.1080/15412555.2020.1782867 (Accessed: 15 September 2025)..
Conclusion
There was consistency in the reports for all patients, which was reassuring in that it suggested that the RPM we had developed was reflective of, and in line with, patient needs and expectations. The most emergent themes: positive user experience with the technology and devices, patient engagement and compliance, and positive impact on patient and provider relationships–provided useful insights into the potential benefits of RPM for asthma monitoring and care.
Funding
None.
Informed Consent Statement
All study procedures were approved by the Baystate Techspring Review Team at Baystate Health (approval 2021-R-015). This study was approved by the compliance and IT teams at Baystate Health. Each study participant read and signed an informed consent form outlining the purpose, risks, and benefits of this study and had the opportunity to ask questions and seek clarification from this study’s staff when reading and signing the form. The informed consent form also described how participation and the resulting data would be kept private and confidential (i.e., all study data were de-identified and stored in either locked drawers or on password-protected servers accessible only to this study’s team). The patients received a US$15 gift card to participate in the interviews.
Data Availability Statement
The data that support the findings of this study are available upon request from the corresponding author, Naomi Rajput (NR). The data are not publicly available because of the small sample size, which could compromise the privacy of research participants.
Acknowledgements
We thank Jennifer P, Joe Diver, Jill McCormick, Christian Lagie, Heather, and Jessye Chalmers for helping with the study setup, strategic guidance, and completion of the study. We would also like to thank Baystate Noble Hospital, which provided us with access to their patients.
Author Contributions
Naomi Rajput is an undergraduate student at Northeastern University pursuing a degree in neuroscience. She has been involved in the development of a remote patient monitoring (RPM) product for the past three years and has worked directly with patients using the technology for clinical monitoring purposes. Naomi led the transcription and thematic coding of interviews using NVivo, applying qualitative analytic methods and statistical techniques informed by her prior research experience. She also led the development and refinement of the study methodology, contributing to conceptual design, data curation, and original draft preparation.
Jyotsna Mehta, MS, holds a master's degree in pharmacy and health economics. She has extensive research and clinical experience in healthcare technology and chronic disease management. Jyotsna supported data analysis and manuscript review, drawing on her background in health economics and chronic care. Her contributions helped validate findings and strengthen methodological rigor.
Kathryn Lasch, PhD, is a subject matter expert in Clinical Outcome Assessments (COAs) and Patient Reported Outcomes (PROs). Her guidance was instrumental in developing the semi-structured interview guide and structuring the data collection and analysis processes. Dr. Lasch conducted all patient interviews and supervised the research team to ensure methodological integrity and ethical compliance.
Denzil Reid, MD, is a practicing pulmonologist with extensive clinical experience. He contributed essential insights to ensure the clinical relevance of the research and provided access to patients under his care, enriching the study with real-world clinical perspectives.
All authors, except for Denzil Reid, the clinician who facilitated patient access, had no prior relationship with the participants. This co-author also did not participate in data collection or analysis. The interdisciplinary backgrounds of the team enriched the study by bringing together expertise in patient care, digital health, research methodology, and patient-centered outcomes. This diversity strengthened the analysis, ensuring it was both clinically meaningful and methodologically robust. All authors have read and approved the final manuscript.
Formal Contributions (CRediT taxonomy):
- Naomi Rajput, BS: Conceptualization, Data Curation, Formal Analysis, Investigation, Methodology (lead), Software, Transcription, Thematic Coding, Writing – Original Draft, Visualization
- Jyotsna Mehta, MS: Conceptualization, Validation, Writing – Review & Editing, Supervision
- Kathryn Lasch, PhD: Conceptualization, Investigation, Methodology, Supervision, Writing – Review & Editing
- Denzil Reid, MD: Resources, Supervision
Declaration of conflicting interests
The authors declare the following competing interests: Dr. Reid, affiliated with Baystate, contributed to the study design. Jyotsna Mehta, affiliated with Keva Health, is the developer of the product evaluated in this study. The authors declare no other competing interests related to the research, authorship, or publication of this article.
References
- Reid, D.M., Mehta, J., Mehta, S., Divgi, V.D. and Anis, K.H. (2022) ‘Clinically meaningful data from remote spirometry monitoring in asthma management in a US-based observational study’, Chest, 162(4), p. A2474. doi:10.1016/j.chest.2022.08.2026. Available at: https://doi.org/10.1016/j.chest.2022.08.2026 (Accessed: 15 September 2025).
- Serrano, L.P., Maita, K.C., Avila, F.R., Torres-Guzman, R.A., Garcia, J.P., Eldaly, A.S., Haider, C.R., Felton, C.L., Paulson, M.R., Maniaci, M.J. and Forte, A.J. (2023) ‘Benefits and challenges of remote patient monitoring as perceived by health care practitioners: A systematic review’, The Permanente Journal, 27(4), pp. 100–111. doi:10.7812/TPP/23.022. Available at: https://doi.org/10.7812/TPP/23.022 (Accessed: 15 September 2025).
- Farnesi, B.C., Ducharme, F.M., Blais, L., Collin, J., Lavoie, K.L., Bacon, S.L., McKinney, M.L. and Peláez, S. (2019) ‘Guided asthma self-management or patient self-adjustment? Using patients’ narratives to better understand adherence to asthma treatment’, Patient Preference and Adherence, 13, pp. 587–597. doi:10.2147/PPA.S195585. Available at: https://doi.org/10.2147/PPA.S195585 (Accessed: 15 September 2025).
- Shah, S.A., Quint, J.K. and Sheikh, A. (2022) ‘Impact of COVID-19 pandemic on asthma exacerbations: Retrospective cohort study of over 500,000 patients in a national English primary care database’, The Lancet Regional Health – Europe, 19, 100428. doi:10.1016/j.lanepe.2022.100428. (Accessed: 15 September 2025).
- Philip, K.E.J., Buttery, S., Williams, P., Vijayakumar, B., Tonkin, J., Cumella, A., Renwick, L., Ogden, L., Quint, J.K., Johnston, S.L., Polkey, M.I. and Hopkinson, N.S. (2022) ‘Impact of COVID-19 on people with asthma: A mixed methods analysis from a UK-wide survey’, BMJ Open Respiratory Research, 9(1), e001056. doi:10.1136/bmjresp-2021-001056. Available at: https://bmjopenrespres.bmj.com/content/9/1/e001056 (Accessed: 15 September 2025).
- Ogden, L., Quint, J.K., Johnston, S.L., Polkey, M.I. and Hopkinson, N.S. (2022) ‘Impact of COVID-19 on people with asthma: A mixed methods analysis from a UK-wide survey’, BMJ Open Respiratory Research, 9(1), e001056. doi:10.1136/bmjresp-2021-001056. Available at: https://bmjopenrespres.bmj.com/content/9/1/e001056 (Accessed: 15 September 2025).
- Hyder, M. and Razzak, J. (2020) ‘Telemedicine in the United States: An introduction for students and residents’, Journal of Medical Internet Research, 22(11), e20839. doi:10.2196/20839. Available at: https://www.jmir.org/2020/11/e20839(Accessed: 15 September 2025).
- Reid, D., Mehta, J., Anis, K. and Mehta, S. (2023) ‘Impact of remote patient monitoring platform on patients with moderate to severe persistent asthma: Observational study’, JMIR Formative Research, 7, e51065. doi:10.2196/51065. Available at: https://formative.jmir.org/2023/1/e51065 (Accessed: 15 September 2025).
- Centers for Disease Control and Prevention (2023) Asthma surveillance in the U.S., 2001–2021. Atlanta, GA: Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/asthma/asthma-prevalence-us-2023-508.pdf(Accessed: 15 September 2025).
- Centers for Disease Control and Prevention (2023) Most recent national asthma data. Atlanta, GA: Centers for Disease Control and Prevention. Updated 17 June 2024. Available at: https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm (Accessed: 15 September 2025).
- Miller, R.L., Breysse, P.N., Jacobs, D.E., Kanchanaraksa, S., Morley, R.L., Sampson, N.R. and Svendsen, E.R. (2021) ‘Impact of the COVID-19 pandemic on asthma exacerbations in the United States: Insights from electronic health records and remote patient monitoring’, Journal of Allergy and Clinical Immunology: In Practice, 9(8), pp. 2903–2913. doi:10.1016/j.jaip.2021.06.034.
- Coffey, J.D., Christopherson, L.A., Glasgow, A.E., Pearson, K.K., Brown, J.K., Gathje, S.R., Sangaralingham, L.R., Carmona Porquera, E.M., Virk, A., Orenstein, R., Speicher, L.L., Bierle, D.M., Ganesh, R., Cox, D.L., Blegen, R.N. and Haddad, T.C. (2021) ‘Implementation of a multisite, interdisciplinary remote patient monitoring program for ambulatory management of patients with COVID-19’, NPJ Digital Medicine, 4(1), 123. doi:10.1038/s41746-021-00490-9. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC8363637/ (Accessed: 15 September 2025).
- Fusi-Schmidhauser, T., Froggatt, K. and Preston, N. (2020) ‘Living with advanced chronic obstructive pulmonary disease: A qualitative interview study with patients and informal carers’, COPD: Journal of Chronic Obstructive Pulmonary Disease, 17(4), pp. 410–418. doi:10.1080/15412555.2020.1782867. Available at: https://doi.org/10.1080/15412555.2020.1782867 (Accessed: 15 September 2025).
- Delameillieure, A., Dobbels, F., Vandekerkhof, S. et al. (2021) ‘Patients’ and healthcare professionals’ perspectives on the idiopathic pulmonary fibrosis care journey: A qualitative study’, BMC Pulmonary Medicine, 21, 93. doi:10.1186/s12890-021-01431-8. Available at: https://doi.org/10.1186/s12890-021-01431-8 (Accessed: 15 September 2025).
- Genberg, E.M., Viitanen, H.T., Mäkelä, M.J. et al. (2023) ‘Impact of a digital web-based asthma platform, a real-life study’, BMC Pulmonary Medicine, 23, 165. doi:10.1186/s12890-023-02467-8. Available at: https://doi.org/10.1186/s12890-023-02467-8 (Accessed: 15 September 2025).
- L, S.P., Khurdi, S., G, P.T. and Mary, S.P. (2024) ‘Impact of remote patient monitoring systems on nursing time, healthcare providers, and patient satisfaction in general wards’, Cureus, 16(6), e61646. doi:10.7759/cureus.61646. Available at: https://doi.org/10.7759/cureus.61646 (Accessed: 15 September 2025).
- Caneiras, C., Jácome, C., Moreira, E., Oliveira, D., Dias, C.C., Mendonça, L., Mayoralas-Alises, S., Fonseca, J.A., Diaz-Lobato, S., Escarrabill, J. and Winck, J.C. (2022) ‘A qualitative study of patient and carer experiences with home respiratory therapies: Long-term oxygen therapy and home mechanical ventilation’, Pulmonology, 28(4), pp. 268–275. doi:10.1016/j.pulmoe.2021.05.010. Available at: https://doi.org/10.1016/j.pulmoe.2021.05.010 (Accessed: 15 September 2025).
- American Lung Association (2024) Asthma trends brief: Asthma trends and burden. Chicago, IL: American Lung Association. Available at: https://www.lung.org/research/trends-in-lung-disease/asthma-trends-brief/trends-and-burden(Accessed: 15 September 2025).
- American Medical Association (2024) Remote patient monitoring implementation playbook overview. Chicago, IL: American Medical Association. Available at: https://www.ama-assn.org/practice-management/digital/remote-patient-monitoring-implementation-playbook-overview (Accessed: 15 September 2025).
- Jackson, K. and Bazeley, P. (2019) Qualitative data analysis with NVivo. 3rd edn. Thousand Oaks, CA: Sage. Available at: https://us.sagepub.com/sites/default/files/upm-assets/114916_book_item_114916.pdf (Accessed: 15 September 2025).
- Jackson, K. and Bazeley, P. (2019) Qualitative data analysis with NVivo. 3rd edn. Thousand Oaks, CA: Sage. Available at: https://us.sagepub.com/sites/default/files/upm-assets/114916_book_item_114916.pdf (Accessed: 15 September 2025).
Abbreviations
The following abbreviations are used in this manuscript:
RPM Remote Patient Monitoring
CDC Centers for Disease Control and Prevention
COAs Clinical Outcome Assessments
PROs Patient Reported Outcomes
HIPAA Health Insurance Portability and Accountability Act
ATAQ The Asthma Therapy Assessment Questionnaire
Appendix
Appendix A.1
- Open-ended Guide:
- Do you find the KevaTalk app (formerly known as Asthma Advisor app) easy or difficult to use?
i. If easy – What do you find easy about it?
ii. If difficult – What do you find difficult?
iii. Is the app easy to navigate?
iv. What issues, if any, did you encounter while using the app?
B. Tell me about what it was like for you to connect the spirometer to the Asthma Advisor
application?
i. Was it easy or difficult to connect the spirometer to the Asthma Advisor application?
1. If easy – What do you find easy about it?
2. If difficult – What do you find difficult about it?
C. What do you like or dislike about the Asthma Advisor application?
i. Are there specific features you like? Why?
ii. Are there any specific features that you do not like?
D. Did you receive regular notifications from the Asthma Advisor application to “check in?”
iSure, continuing from where we left off:
i. If yes, how often did you get a notification?
ii. What do you think about the notifications?
iii. Do you find the notifications helpful?
iv. What did you do when you received a notification?
v. What encourages you to use the app regularly?
Disclaimer/Publisher’s Note: The statements, opinions, and data contained in all publications are solely those of the individual author(s) and contributor(s), and not of MDPI and/or the editor(s). The MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content.
Declarations
Ethics approval and consent to participate
All study procedures were approved by the Baystate Techspring Review Team at Baystate Health (approval 2021-R-015).