


Background
Type 2 Diabetes Mellitus (T2DM) affects around 34.2 million people in the U.S., or 10.5% of the population [1]Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020. [Internet]. Atlanta, GA: U.S. Department of Health and Human Services; 2020. Available from: https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf. Accessed 02 November 2023, and is the leading cause of chronic kidney disease (CKD) [2]Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2019. Atlanta, GA: US Department of Health and Human Services. Centers for Disease Control and Prevention; 2019.[3]National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Chronic Kidney Disease. National Institute of Diabetes and Digestive and Kidney Diseases, U.S. Department of Health and Human Services, [Updated 2023-08-04]. Accessed 2023-11-04. URL: https://www.niddk.nih.gov/health-information/kidney-disease/chronic-kidney-disease-ckd. About 40% of adults with T2DM have some degree of CKD [4]Koro CE, Lee BH, Bowlin SJ. Antidiabetic medication use and prevalence of chronic kidney disease among patients with type 2 diabetes mellitus in the United States. Clinical therapeutics. 2009 Nov 1;31(11):2608-17.. T2DM has unique mechanisms like insulin resistance and metabolic syndrome that speed up CKD progression. Research [5]Alicic RZ, Rooney MT, Tuttle KR. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin J Am Soc Nephrol. 2017;12(12):2032-2045. doi:10.2215/CJN.11491116 has shown that diabetic kidney disease (DKD) in T2DM patients causes albuminuria, declining kidney function, and increased cardiovascular risks. CKD in T2DM patients also raises the risk of heart problems and death. Socio-demographic factors, especially in minority populations, affect outcomes, with non-Hispanic Black and Native American groups facing worse results due to healthcare inequities [6]Bruce MA, Beech BM, Crook ED, Sims M, Wyatt SB, Flessner MF, Taylor HA, Williams DR. "Social determinants of health in African Americans with end-stage renal disease." Clin J Am Soc Nephrol. 2010;5(6):1115-1129. doi:10.2215/CJN.05961109.. Most studies focus on advanced CKD or end-stage renal disease (ESRD), but early-to-moderate stages, where intervention can help, are often overlooked.
Objective
To determine mortality trends for T2DM-associated CKD from 1999 to 2020 among adults in the United States, emphasizing early-to-moderate CKD stages to highlight opportunities for early intervention.
Methods
In December 2024, data on CKD-related deaths among patients with T2DM in the United States was collected from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research database (CDC WONDER) [7]About multiple causes of death, 1999-2020. Accessed September 01, 2023.https://wonder.cdc.gov/mcd-icd10.html. Death certificates were used to identify CKD and T2DM with ICD-10-CM codes (E11 for T2DM, N18 for CKD). The data was categorized into two age groups: young (25–64 years) and older (>64 years). Institutional review board approval was not needed as the data was de-identified. Data collected included year, population size, demographics, CKD stage, geographic regions, and urban-rural classification. CKD severity was divided into early (stages 1-2), moderate (stages 3-4), and advanced (stage 5 or ESRD). Demographics included age, race/ethnicity, and gender. Urban and rural areas were classified by the National Center for Health Statistics. Crude and age-adjusted mortality rates (AAMRs) per 1,000,000 individuals were calculated. Trends in AAMRs were assessed using Joinpoint regression, and annual percent changes (APCs) were determined with 95% confidence intervals (CIs). Statistical significance was set at p< 0.05.
The inclusion criteria included adults aged 25 years and older with CKD listed as a cause of death and T2DM as an underlying or contributing cause. Only deaths occurring in the United States between 1999 and 2020 were included. Additionally, individuals with complete demographic and geographic information in the dataset were considered. The exclusion criteria comprised patients without documented CKD or T2DM on the death certificate, pediatric populations under 25 years, and cases with missing or incomplete data regarding key variables such as age, sex, or geographic classification.
Results
There were a total of 90,615 CKD-related deaths among adults with T2DM between 1999 and 2020. The AAMR was 15.0 in 1999, which increased to 26.0 by 2009 (APC: 4.20; 95% CI: 1.98-6.48), after which there was a sharp rise to 56.0 by 2012 (APC: 20.5; 95% CI: -0.03-45.28). It then gradually declined to 3.6 (95% CI: 2.8–4.5) in 2015. By 2020, the AAMR steadily rose to 7.5 (APC: 30.5, 95% CI: 18.91-43.2). The AAMRs for men were higher than those for women throughout the years (23.2 with 95% CI of 22.96–23.39 vs.16.1 with 95% CI of 15.97–16.28). NH American Indian or Alaska Native patients had the highest AAMR (56.2, 95% CI: 53.2–59.2]), followed by NH Black or African American (32.0, 95% CI: 31.5–32.6), Hispanic or Latino (28.7, 95% CI: 28.1–29.3), NH Asian or Pacific Islander (16.6, 95% CI: 16.0–17.2), and NH White populations (16.2, 95% CI: 16.1–16.4). Nonmetropolitan areas experienced a relatively greater mortality burden with higher AAMR (23.3, 95% CI: 23.5–24.2) compared to metropolitan areas (16.9, 95% CI: 17.8–18.1), while the Western region had the highest overall AAMR (22.8, 95% CI: 22.5–23.1), followed by the Midwestern (22.1, 95% CI: 21.8–22.4), Southern (18.0, 95% CI: 17.8–18.2), and Northeastern (12.9, 95% CI: 12.7–13.1) regions. Early CKD stages (Stages 1 and 2) showed lower mortality rates, with age-adjusted mortality rates (AAMR) significantly lower than those for later stages. For example, in 2015, the AAMR for individuals in Stage 1 was 3.6 (95% CI: 2.8-4.4), compared to 56.0 (95% CI: 54.2-57.8) for individuals in later stages (Stages 3-5). CKD stages contributed significantly to overall mortality, particularly among minority populations and non-metropolitan areas, underscoring the importance of early detection and management strategies.
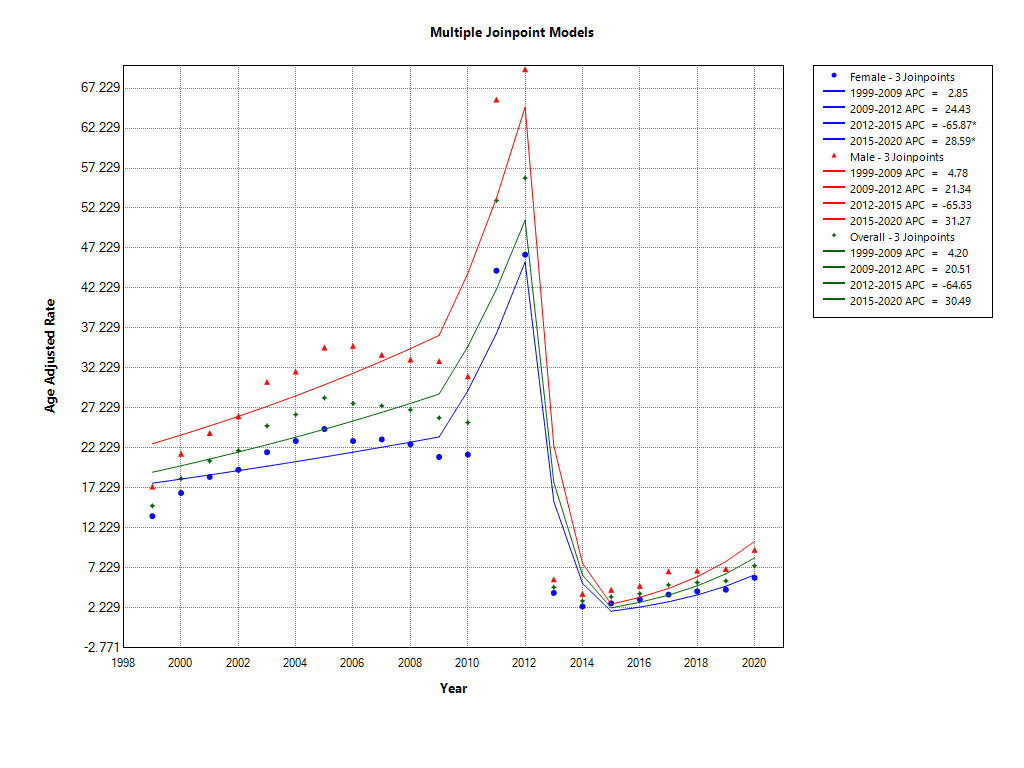
Figure 1 Gender disparities in AAMR trends
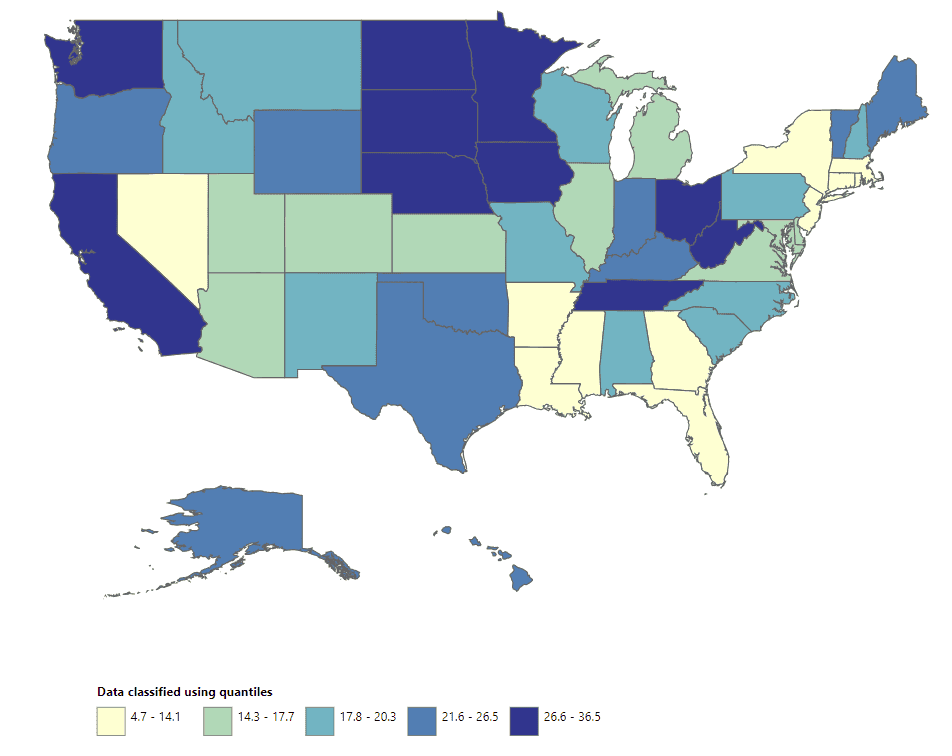
Figure 2 Geographic disparities in mortality burdens
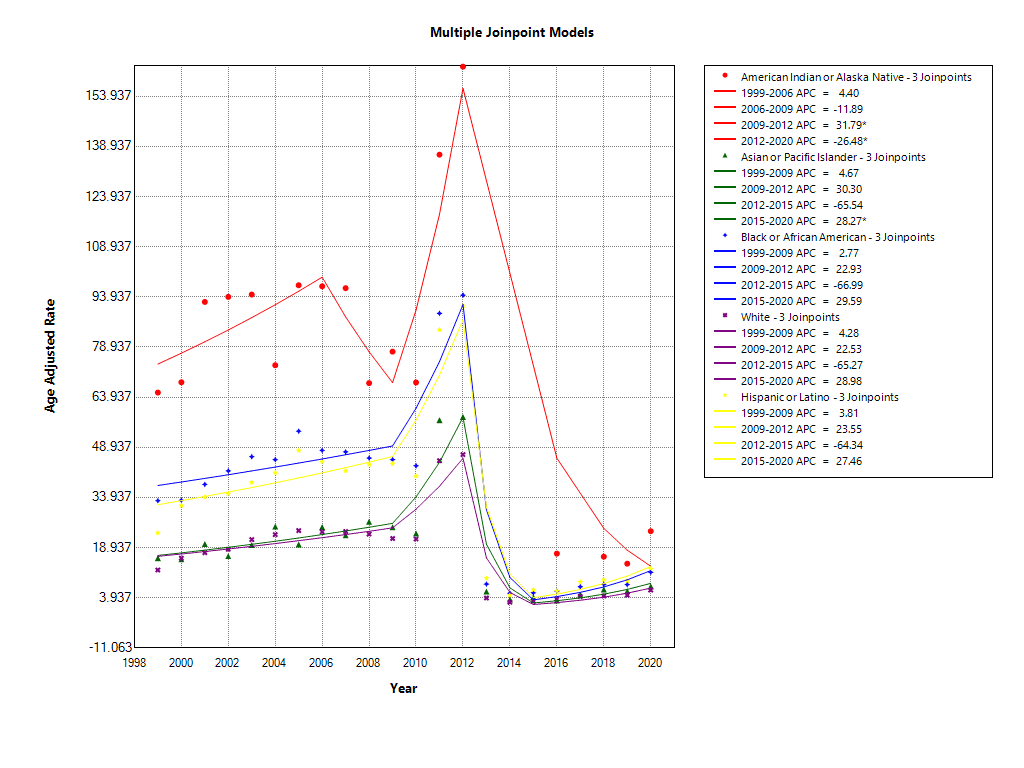
Figure 3 Racial disparities in AAMR trends
Discussion
Our study found several key trends in CKD and T2DM mortality: First, advanced CKD stages had the highest mortality rates. Mortality increased from 1999 to 2012, declined until 2015, and then rose again from 2015 to 2020. Although the increase in AAMR from 2009 to 2012 was not statistically significant, it may still have practical relevance, as it aligns with broader public health concerns such as rising comorbidities, healthcare disparities, and changes in diagnostic practices. Future research with larger datasets or alternative analytical approaches could further clarify whether this trend represents a true shift in CKD-related mortality among T2DM patients. Men had higher mortality rates than women. Native American and Alaska Native populations had the highest mortality, and non-metropolitan areas had more deaths than metropolitan ones. Mortality rates varied by state, with the Western U.S. showing the highest and the Northeast the lowest.
Mortality trends suggest improvements from 2012 to 2015, possibly due to better management of risk factors like hypertension, particularly with the use of SGLT2 inhibitors, which have been shown to improve kidney outcomes in Type 2 diabetes patients [8]Wanner Ch, Inzucchi SE, Zinman B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N Engl J Med. 2016;375(18):1801-1802. doi:10.1056/NEJMc1611290. However, mortality increased after 2015, which may be attributed to factors such as changes in healthcare access, socioeconomic disparities, or a deterioration in the management of risk factors and dietary habits. Early CKD stages showed lower mortality, emphasizing the importance of early intervention. Medications like SGLT2 inhibitors, which help slow CKD progression, are key in these stages [8]Wanner Ch, Inzucchi SE, Zinman B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N Engl J Med. 2016;375(18):1801-1802. doi:10.1056/NEJMc1611290. We also found racial disparities, with Native Americans and African Americans facing higher mortality rates, consistent with previous studies [9]Jolly SE, Burrows NR, Chen SC, Li S, Jurkovitz CT, Norris KC, et al. Racial and Ethnic Differences in Mortality among Individuals with Chronic Kidney Disease: Results from the Kidney Early Evaluation Program (KEEP). Clin J Am Soc Nephrol CJASN. 2011 Aug;6(8):1858–65.[10]Carter JS, Wiggins CL, Becker TM, Key CR, Samet JM. Diabetes Mortality Among New Mexico’s American Indian, Hispanic, and Non-Hispanic White Populations, 1958–1987. Diabetes Care. 1993 Jan 1;16(1):306–9. . This is influenced by increased burden of comorbidities like diabetes mellitus, poorly controlled blood pressure, obesity, and liver diseases [9]Jolly SE, Burrows NR, Chen SC, Li S, Jurkovitz CT, Norris KC, et al. Racial and Ethnic Differences in Mortality among Individuals with Chronic Kidney Disease: Results from the Kidney Early Evaluation Program (KEEP). Clin J Am Soc Nephrol CJASN. 2011 Aug;6(8):1858–65.[11]Acton KJ, Ríos Burrows N, Moore K, Querec L, Geiss LS, Engelgau MM. Trends in Diabetes Prevalence Among American Indian and Alaska Native Children, Adolescents, and Young Adults. Am J Public Health. 2002 Sep;92(9):1485–90.[12]United States: Civil Rights Commission, United States Commission on Civil Rights: Office of the General Counsel. Native American Health Care Disparities Briefing: Executive Summary [Internet]. Civil Rights Commission; 2004 [cited 2023 Nov 10]. Available from: https://purl.fdlp.gov/GPO/LPS51665, social determinants of health, healthcare access, and genetic predispositions as contributors to these disparities. Early CKD stages offer opportunities for intervention to prevent further progression, highlighting the importance of screening, lifestyle changes, and medication.
Limitations include reliance on death certificate data and lack of detailed clinical information. Additionally, unmeasured confounders such as socioeconomic status and healthcare access may impact outcomes. Missing data on key variables like medication use may limit the completeness of the analysis. Lastly, findings may not be generalizable to non-U.S. populations with different healthcare practices. Future research should incorporate cohort-based analyses and explore the impact of emerging therapies, such as finerenone and dual GLP-1 receptor agonists, on CKD outcomes in T2DM.
Conclusions
The highest mortality was seen in men, American Indians, or Alaska Natives, as well as those living in the Western region and non-metropolitan areas. This study highlights the entire spectrum of CKD in T2DM patients, with disparities in mortality burden based on gender, race, and geographic region. Emphasizing early detection and targeted interventions is critical to improving outcomes in this vulnerable population.
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020. [Internet]. Atlanta, GA: U.S. Department of Health and Human Services; 2020. Available from: https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf. Accessed 02 November 2023
- Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2019. Atlanta, GA: US Department of Health and Human Services. Centers for Disease Control and Prevention; 2019.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Chronic Kidney Disease. National Institute of Diabetes and Digestive and Kidney Diseases, U.S. Department of Health and Human Services, [Updated 2023-08-04]. Accessed 2023-11-04. URL: https://www.niddk.nih.gov/health-information/kidney-disease/chronic-kidney-disease-ckd
- Koro CE, Lee BH, Bowlin SJ. Antidiabetic medication use and prevalence of chronic kidney disease among patients with type 2 diabetes mellitus in the United States. Clinical therapeutics. 2009 Nov 1;31(11):2608-17.
- Alicic RZ, Rooney MT, Tuttle KR. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin J Am Soc Nephrol. 2017;12(12):2032-2045. doi:10.2215/CJN.11491116
- Bruce MA, Beech BM, Crook ED, Sims M, Wyatt SB, Flessner MF, Taylor HA, Williams DR. "Social determinants of health in African Americans with end-stage renal disease." Clin J Am Soc Nephrol. 2010;5(6):1115-1129. doi:10.2215/CJN.05961109.
- About multiple causes of death, 1999-2020. Accessed September 01, 2023. https://wonder.cdc.gov/mcd-icd10.html
- Wanner Ch, Inzucchi SE, Zinman B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N Engl J Med. 2016;375(18):1801-1802. doi:10.1056/NEJMc1611290
- Jolly SE, Burrows NR, Chen SC, Li S, Jurkovitz CT, Norris KC, et al. Racial and Ethnic Differences in Mortality among Individuals with Chronic Kidney Disease: Results from the Kidney Early Evaluation Program (KEEP). Clin J Am Soc Nephrol CJASN. 2011 Aug;6(8):1858–65.
- Carter JS, Wiggins CL, Becker TM, Key CR, Samet JM. Diabetes Mortality Among New Mexico’s American Indian, Hispanic, and Non-Hispanic White Populations, 1958–1987. Diabetes Care. 1993 Jan 1;16(1):306–9.
- Acton KJ, Ríos Burrows N, Moore K, Querec L, Geiss LS, Engelgau MM. Trends in Diabetes Prevalence Among American Indian and Alaska Native Children, Adolescents, and Young Adults. Am J Public Health. 2002 Sep;92(9):1485–90.
- United States: Civil Rights Commission, United States Commission on Civil Rights: Office of the General Counsel. Native American Health Care Disparities Briefing: Executive Summary [Internet]. Civil Rights Commission; 2004 [cited 2023 Nov 10]. Available from: https://purl.fdlp.gov/GPO/LPS51665